
Occlusion of the portal circulation often leads to the development of centripetal collateral circulation, which encompasses the entire spectrum from cavernous transformation of the v. portae hepatis to portal biliopathy. While cavernous transformation is caused by partial canalization of the thrombosed vein and expansion of the vasa vasorum of the vena portae hepatis, including the periportal plexus, in portal biliopathy, the veins in and around the wall of the bile ducts expand. Saint’s epicholedochal venous plexus is a venous network in the wall of the choledochal duct, common bile duct, right and left bile ducts, connects to other venous systems, such as the paracholedochal plexus (Petren’s), and flows into the v. gastrica dextra, superior mesenteric vein, and directly into the portal vein. The connection with the above-mentioned venous systems thus forms important porto-portal collaterals. In addition to the actual bile ducts, the same system is also present in the cystic duct and in the wall of the gallbladder, but in the wall of the gallbladder, it is often mainly the submucosal venous plexus that is saturated.
In classic portal biliopathy, there is also an increase in obstructive enzymes and elevation of bilirubin, because the dilated varices of the Saint’s plexus compress the bile ducts.
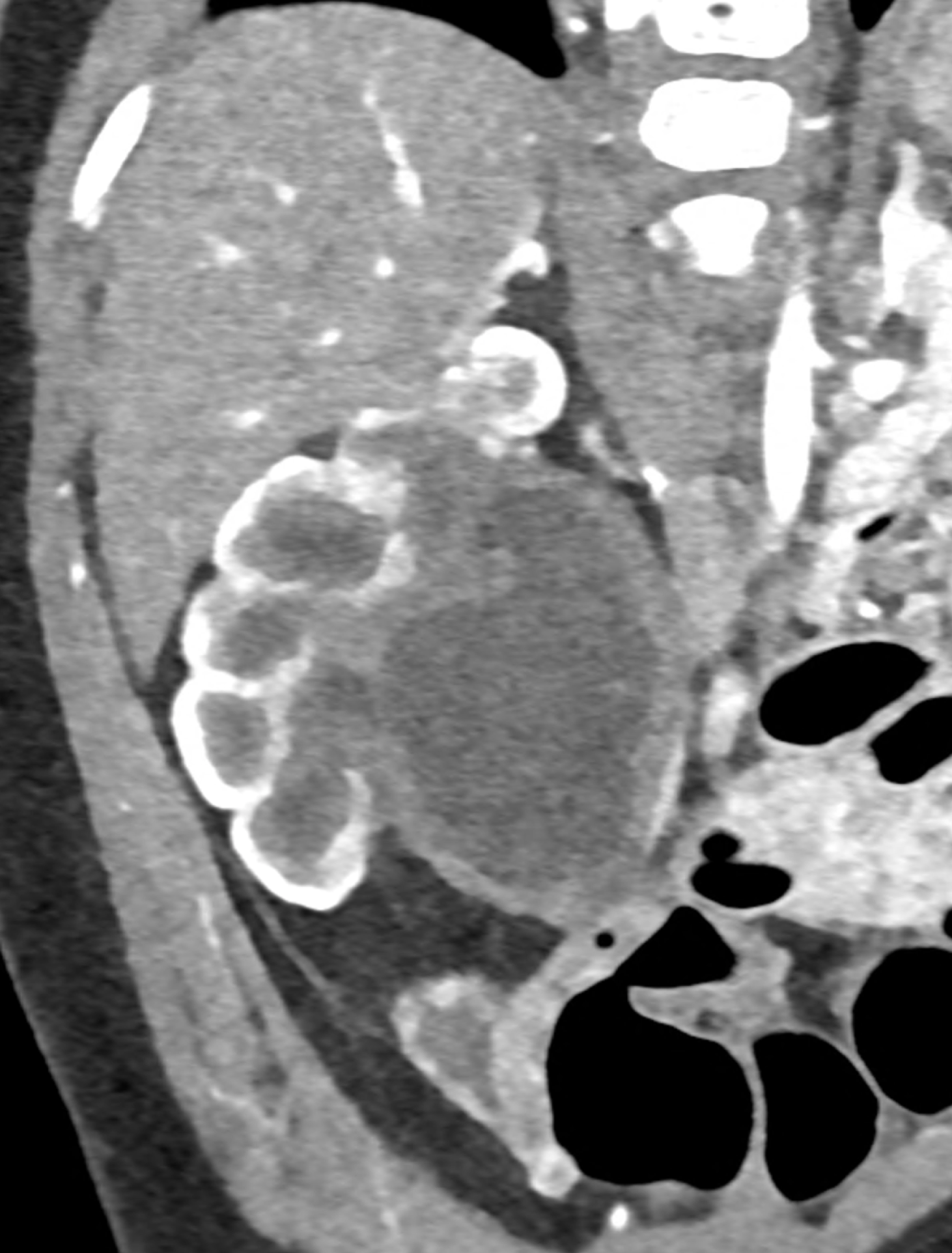
During CT, the most significant phase is the portal phase of liver enhancement, when portal biliopathy is associated with dilation of the bile duct wall, which is significantly enhanced with the contrast agent in the case of dilation of the epicholedochal plexus, or there is a combination with varicose veins around the saturated bile duct wall (dilatation of the paracholedochal plexus). Other possibilities include enhancement of only the paracholedochal plexus and a combination of dilatation of the paracholedochal plexus with cavernous remodelling of the portal vein itself.
The spectral characteristics of data obtained using photon-counting CT allow optimization of the signal from the venous system, thereby increasing the difference between saturated collaterals and the surrounding area. At the same time, excellent spatial resolution aids in the visualization of bile ducts filled with bile.
Case report
A patient with chronic pancreatitis and chronically occluded portal vein. The bile ducts have a significantly dilated wall, from the trunk, through the stump of the cystic duct, to the right and especially the left branch of the hepatic duct. At the same time, a large pseudocyst in the pancreas, dilatation of the pancreatic duct, and chromic occlusion of the superior mesenteric vein, splenic vein, and portal vein trunk are evident. Along with portal biliopathy, there is also arixy of the cardia and esophagus, as well as cavernous remodeling of the portal circulation itself.
Naeotom Alpha.Peak, University Hospital Pilsen, Czechia
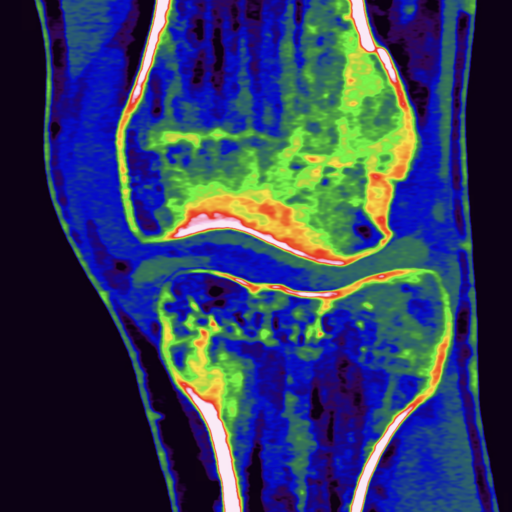
dilated veins in the wall of left hepatic duct

dilated veins in the wall of left hepatic duct and paralel veins of portal cavernous transformation

dilated veins in the wall of cystic duct

dilated collaterals in hepatoduodenal ligament partially portal biliopathy, partially cavernous transformation
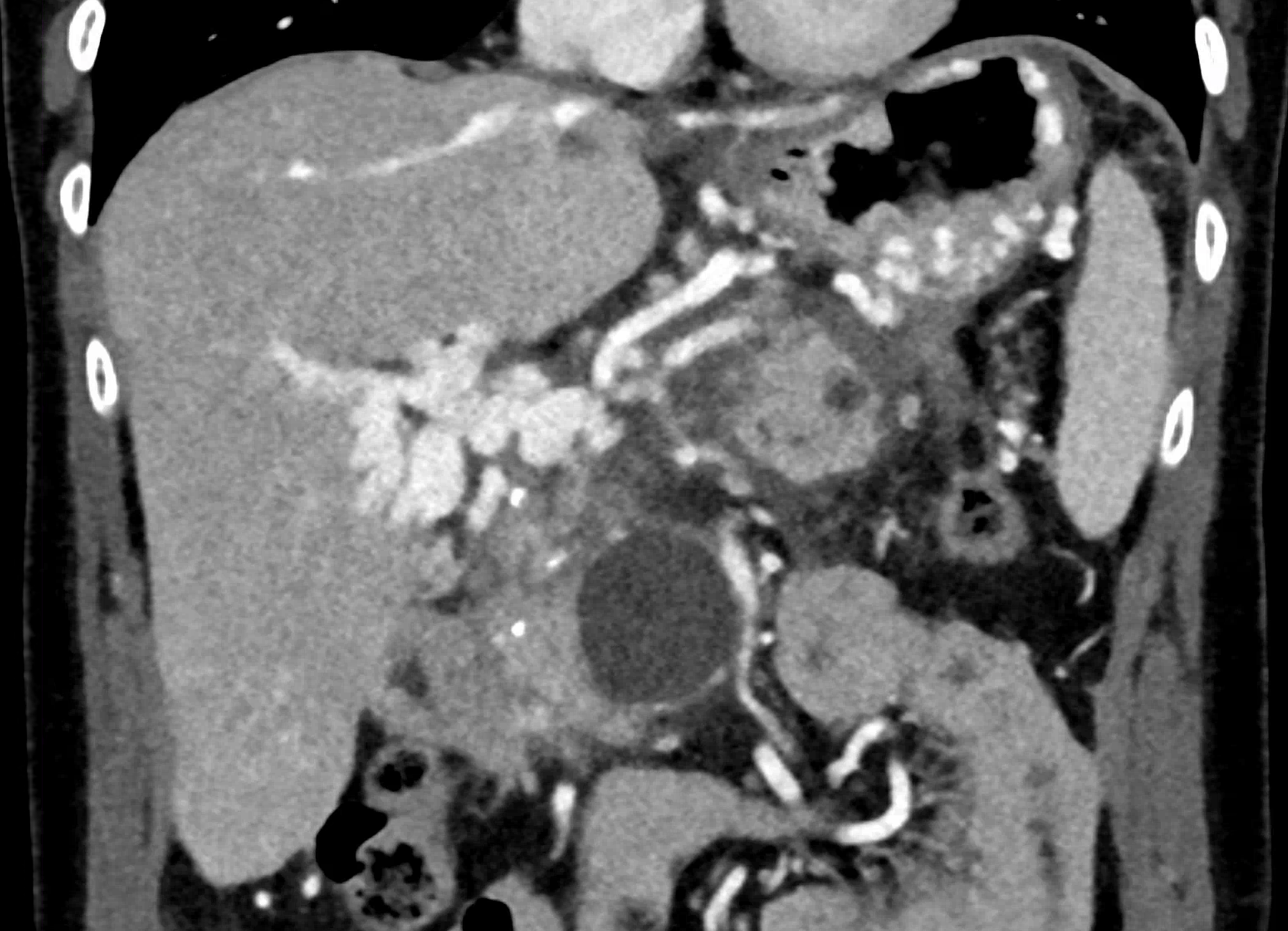
dilated veins in the wall of common hepatic duct
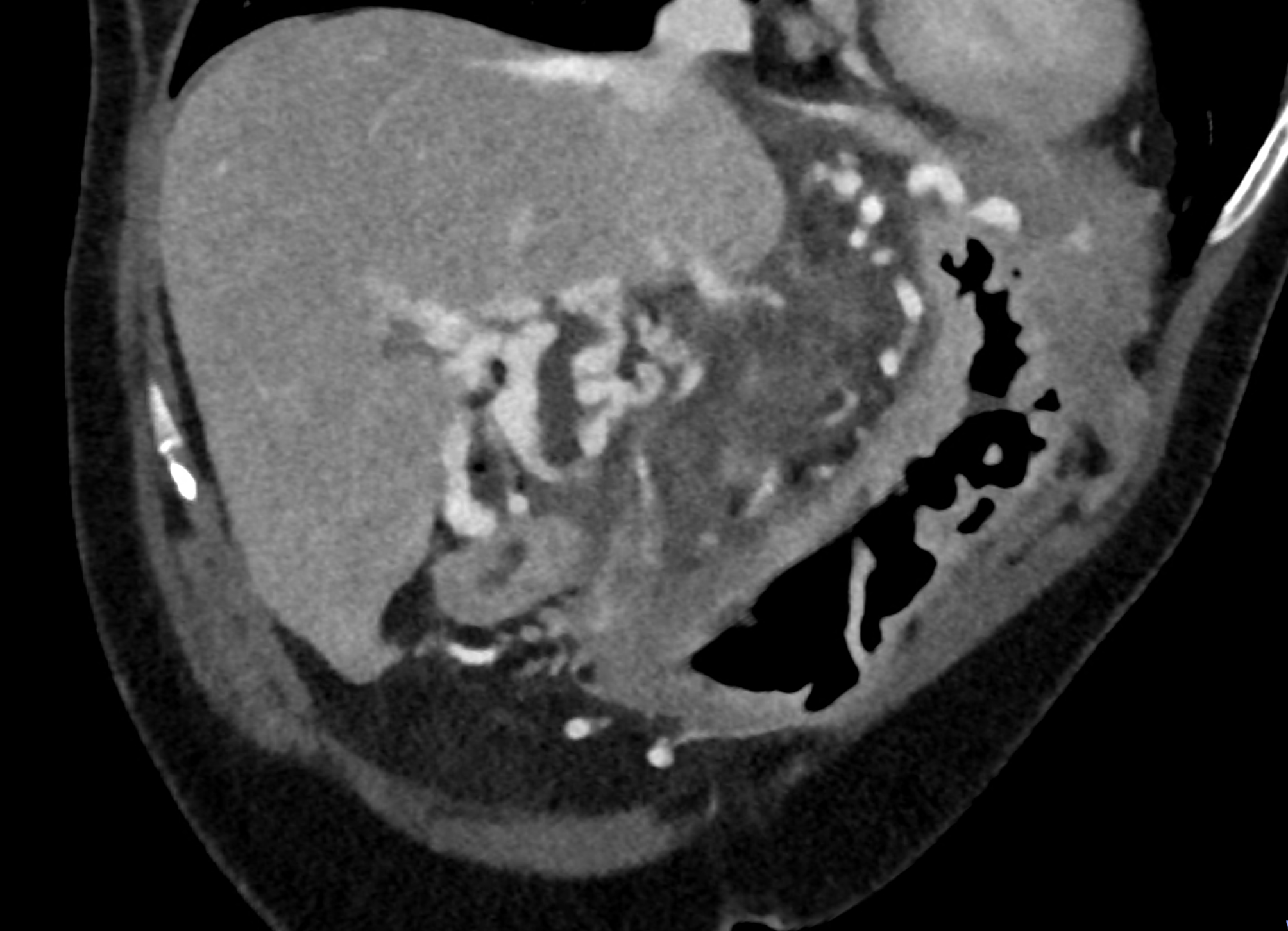
reconstruction paralel to hepatoduodenal ligamant


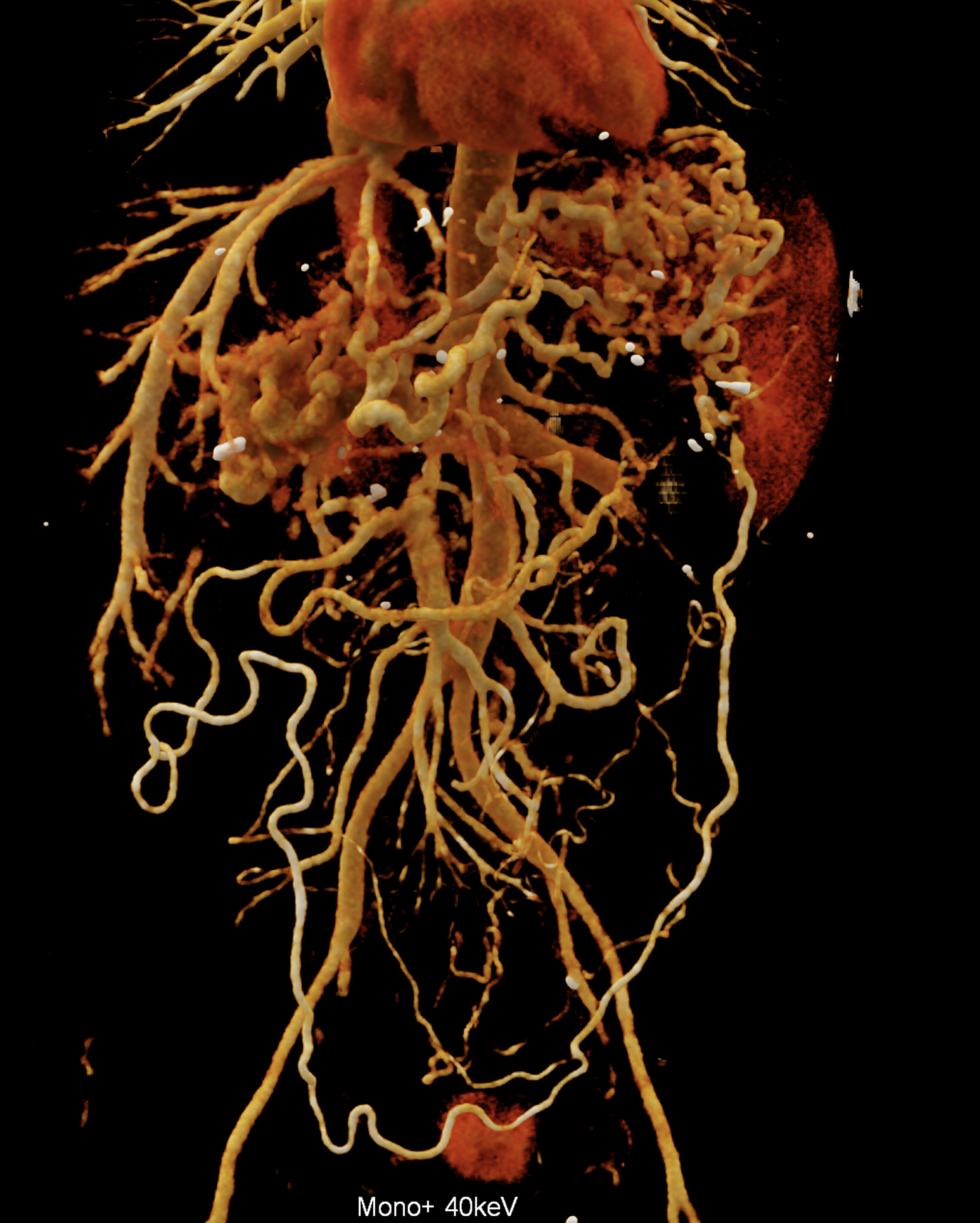
volume rendered image after bone removal
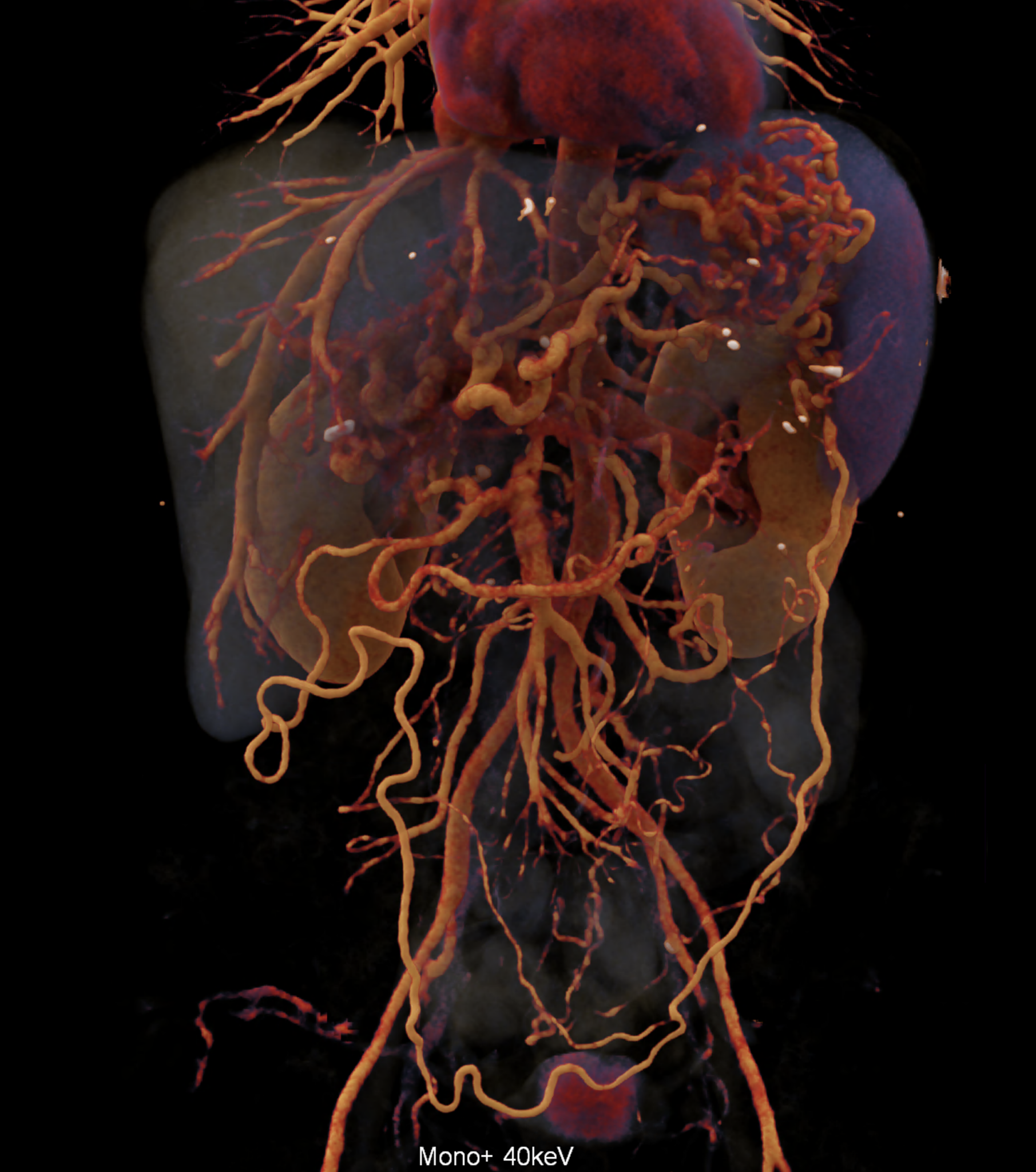
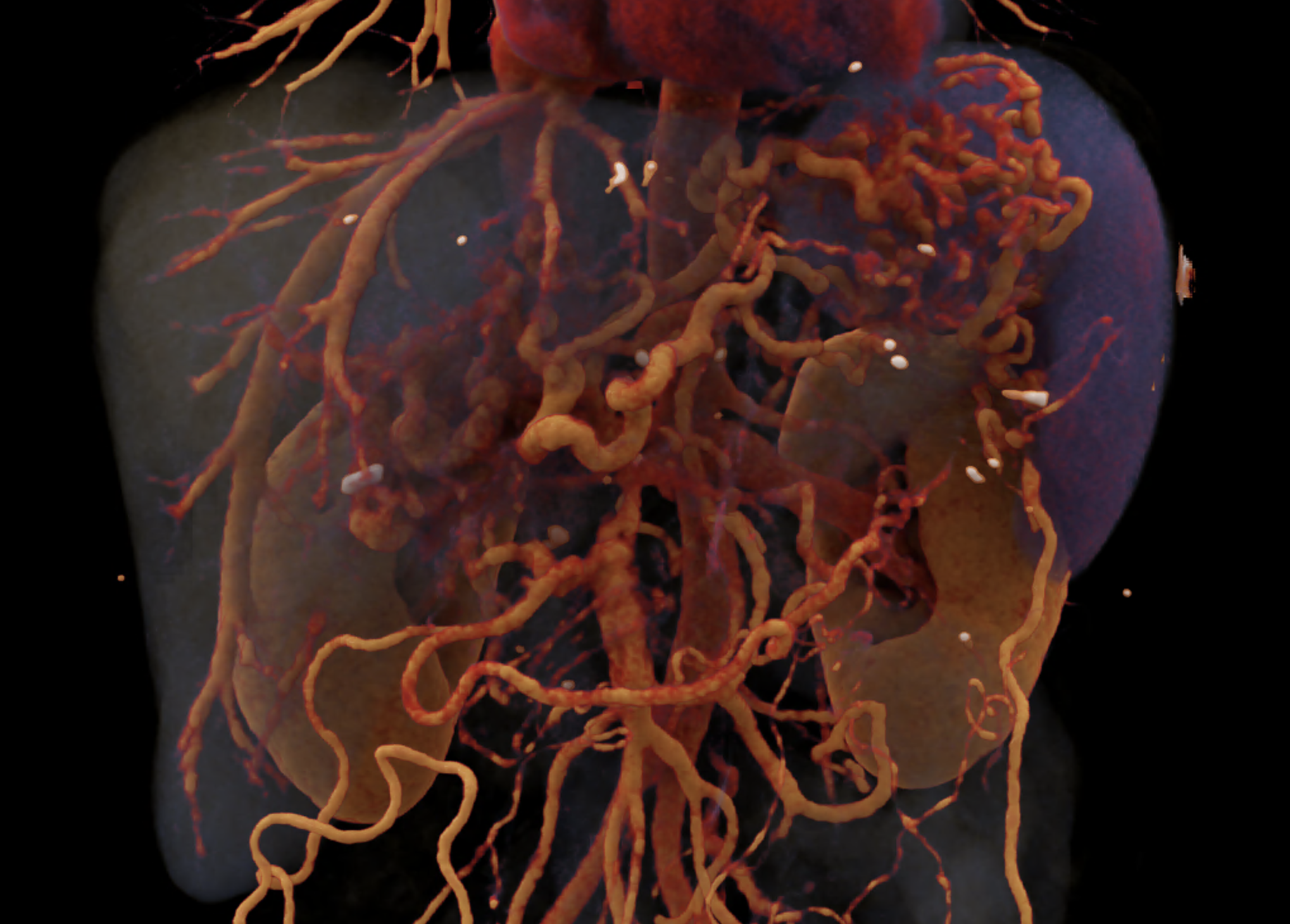
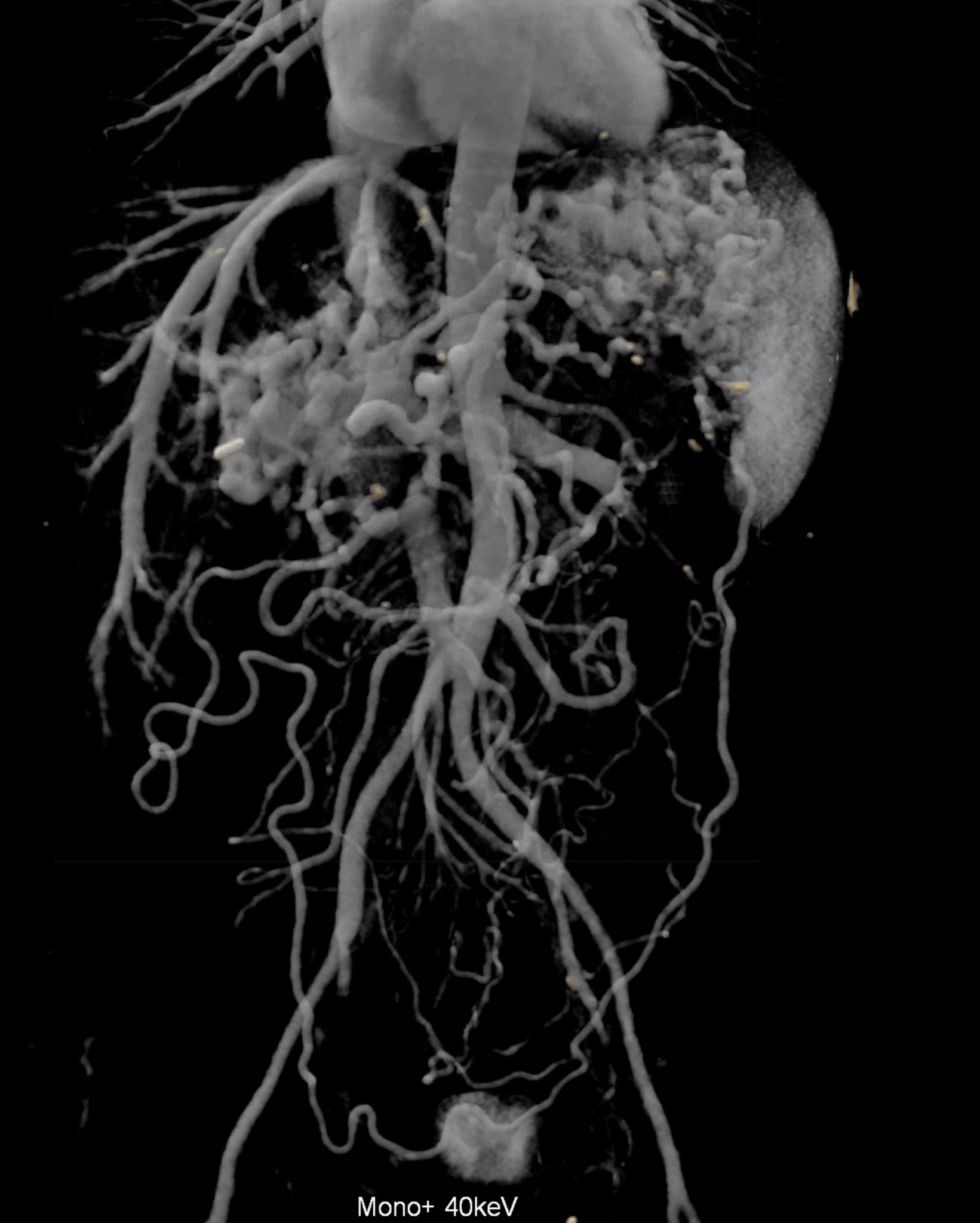
volume rendered image after bone and kidney removal showing best the portal biliopathy