
Budd-Chiari syndrome (BCS) is caused by occlusion of the hepatic veins, leading to hepatic congestion. Common causes include thrombosis, often associated with coagulation disorders such as JAK2 mutation and Leiden mutation. Risk factors also include pregnancy, use of oral contraceptives, and hematological myeloproliferative disorders such as polycythemia vera and essential thrombocythemia. In addition to thrombotic obstruction of the hepatic veins, also known as the radicular type of Budd-Chiari syndrome, compression or occlusion of the hepatic veins by a tumor process is also possible. This type is then called truncal and is caused by hepatocellular or cholangiocellular carcinoma, or occlusion of the hepatic veins by thrombosis of the inferior vena cava, or even occlusion of the hepatic veins or the hepatic segment of the inferior vena cava by a tumor thrombus originating in renal carcinoma. Some features of liver remodelling similar to Budd-Chiari syndrome are also exhibited by the posthepatic type of portal hypertension associated with overpressure in the right-sided compartments in changes falling under the term hepar moschatum (nutmeg liver).
The main clinical symptoms include abdominal pain, hepatomegaly, and ascites, with signs of portal hypertension and sometimes jaundice. Splenomegaly is regularly present.
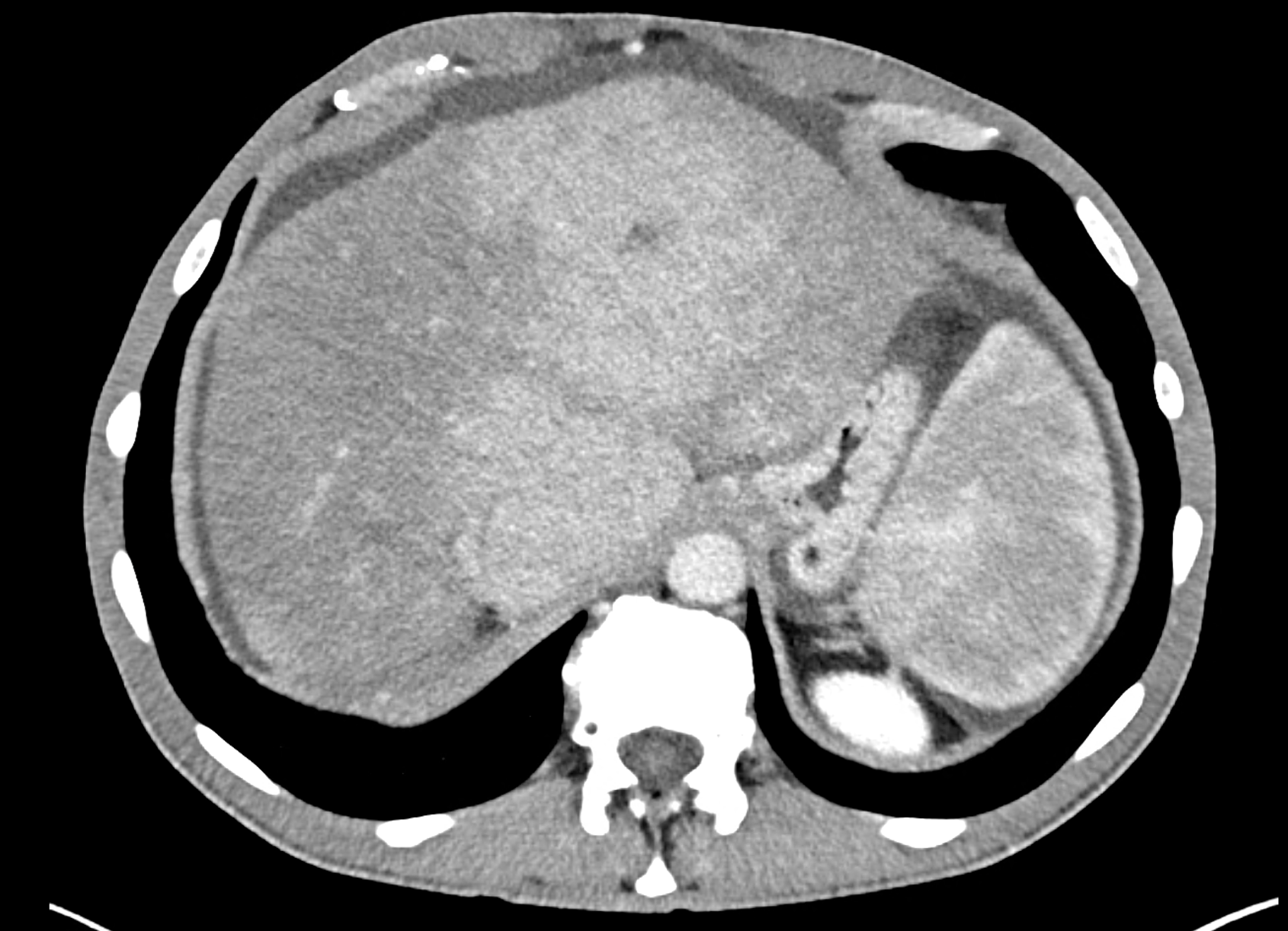
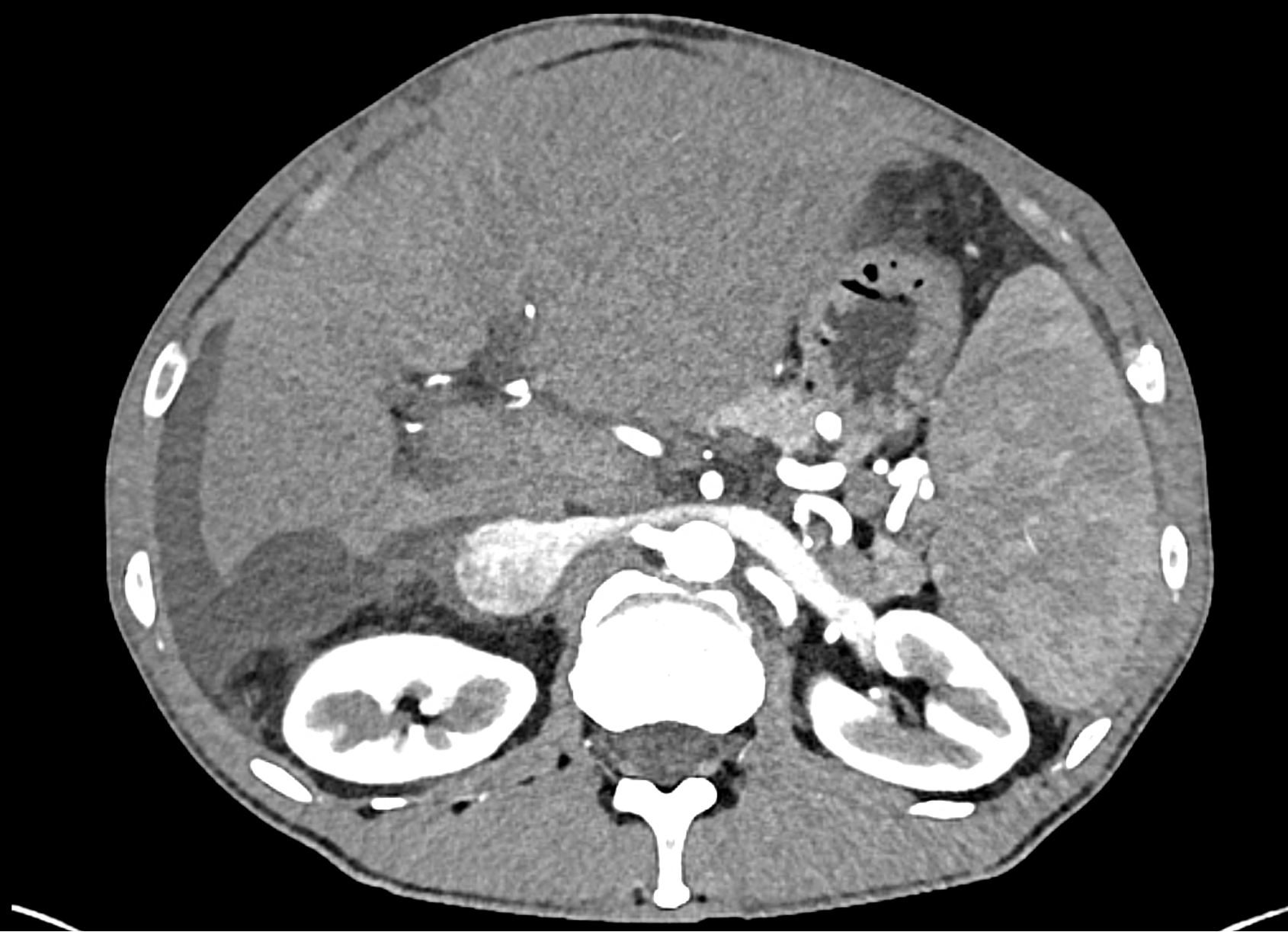
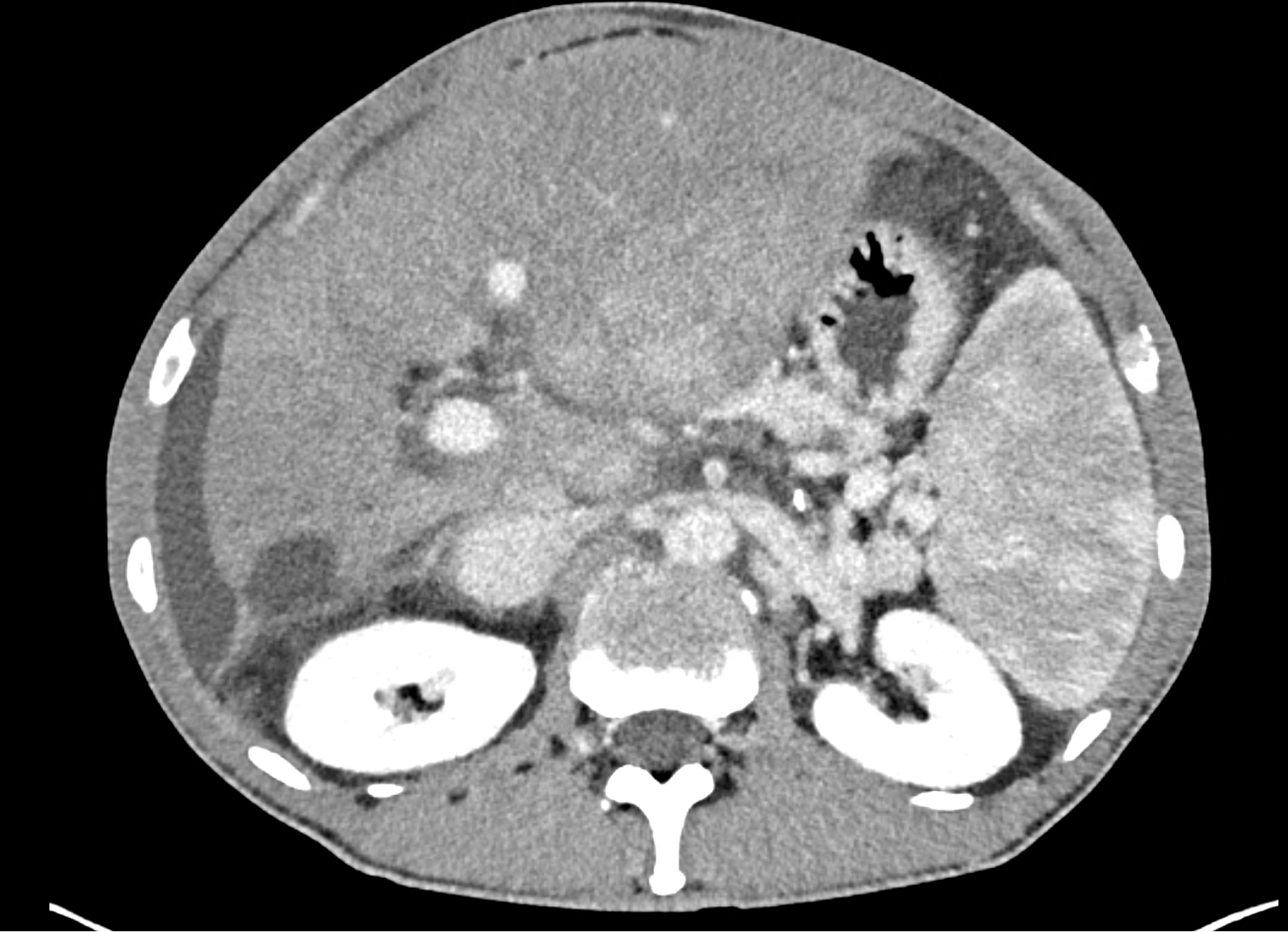
In CT images, BCS manifests as non-homogeneous enhancement of liver tissue in the arterial and especially in the portal phase, although in the portal phase may be increased, especially in the caudate lobe and left lobe, which are often hypertrophic (the hypertrophy and the enhancement is caused due to the possibility of the venous drainage directly into the inferior vena cava through the direct caudate veins), in contrast to the reduction in the right lobe. The portal vein is free, whereas even in the late phase, the hepatic veins and their contrast filling are not visible. Thrombotic occluded veins are hypodense.
In the differential diagnosis, BCS with thrombotic occlusion of the hepatic veins must not be confused with suspected hepatic neoplastic process (bearing in mind, of course, that the invasion of the hepatic veins by a neoplastic process causes similar hemodynamic changes). The presence of ascites and typical changes in the configuration and saturation of the liver are indicative of the classic radicular type. In Budd-Chiari syndrome, the bile ducts are not dilated.
Case report
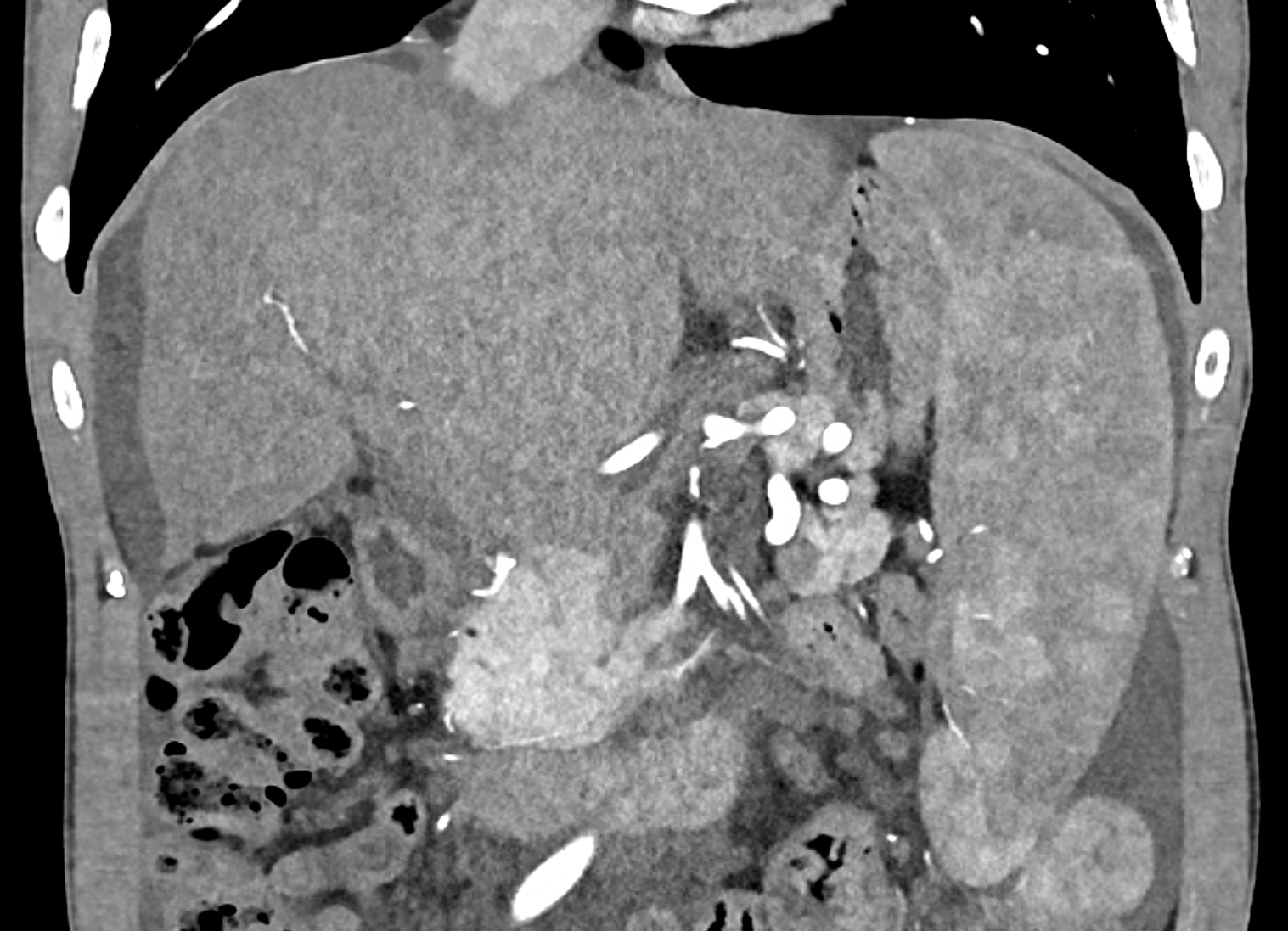
A patient in his sixties with a Leiden mutation of factor V and a heterozygous prothrombin mutation presents with abdominal pain. Ultrasound examination reveals ascites and enlargement of the liver.There is enlargement of the liver, particularly the left lobe and caudate lobe. The hepatic veins are centrally filled with contrast medium due to reflux at the confluence with the inferior vena cava, and their radicular parts are thrombosed. There is typical chronic liver remodelling and the formation of centrifugal collateral circulation, including esophageal varices, and ascites is present in the abdominal cavity.
Naeotom ALpha.Peak, University Hospital Pilsen, Czechia
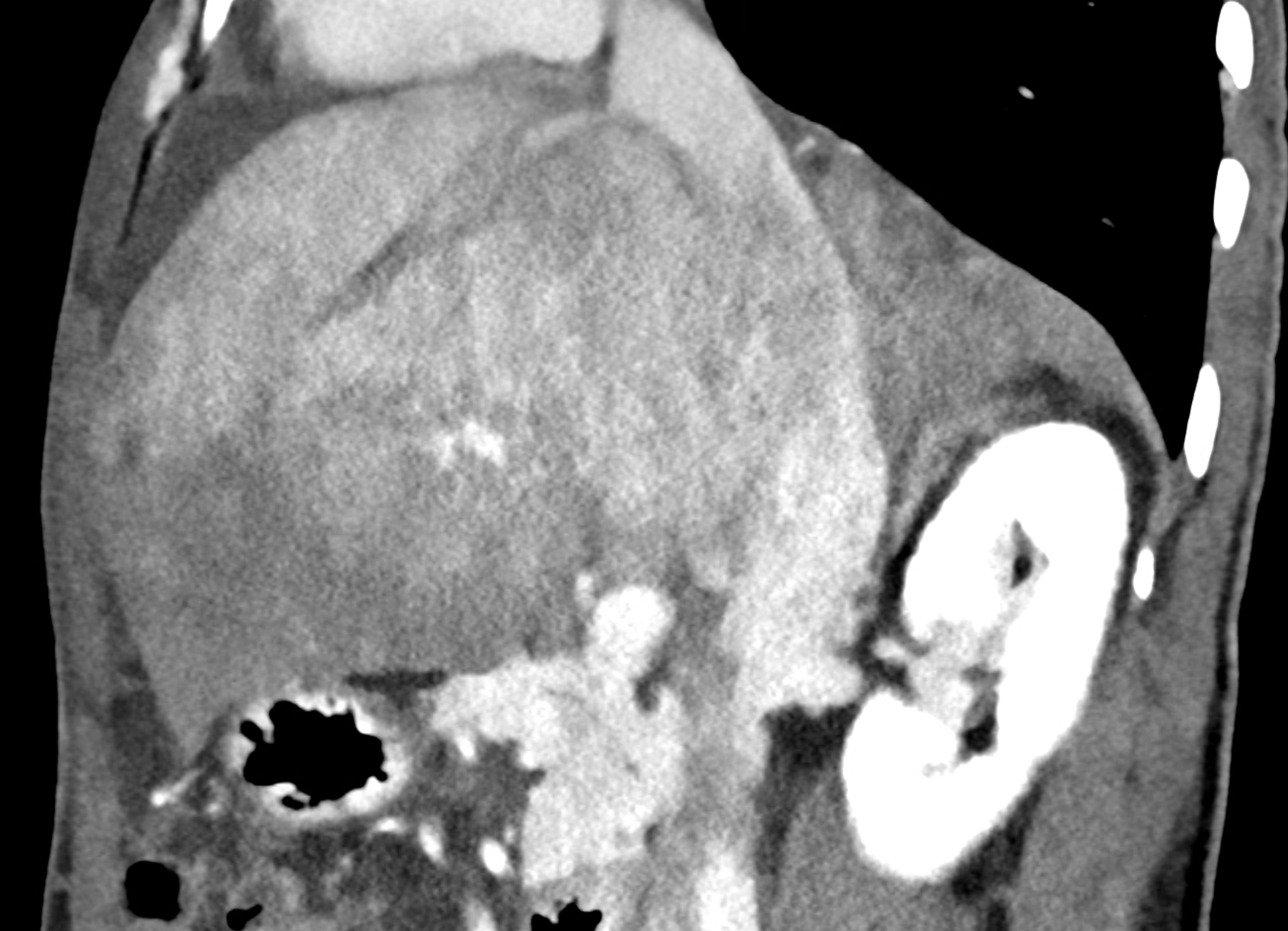
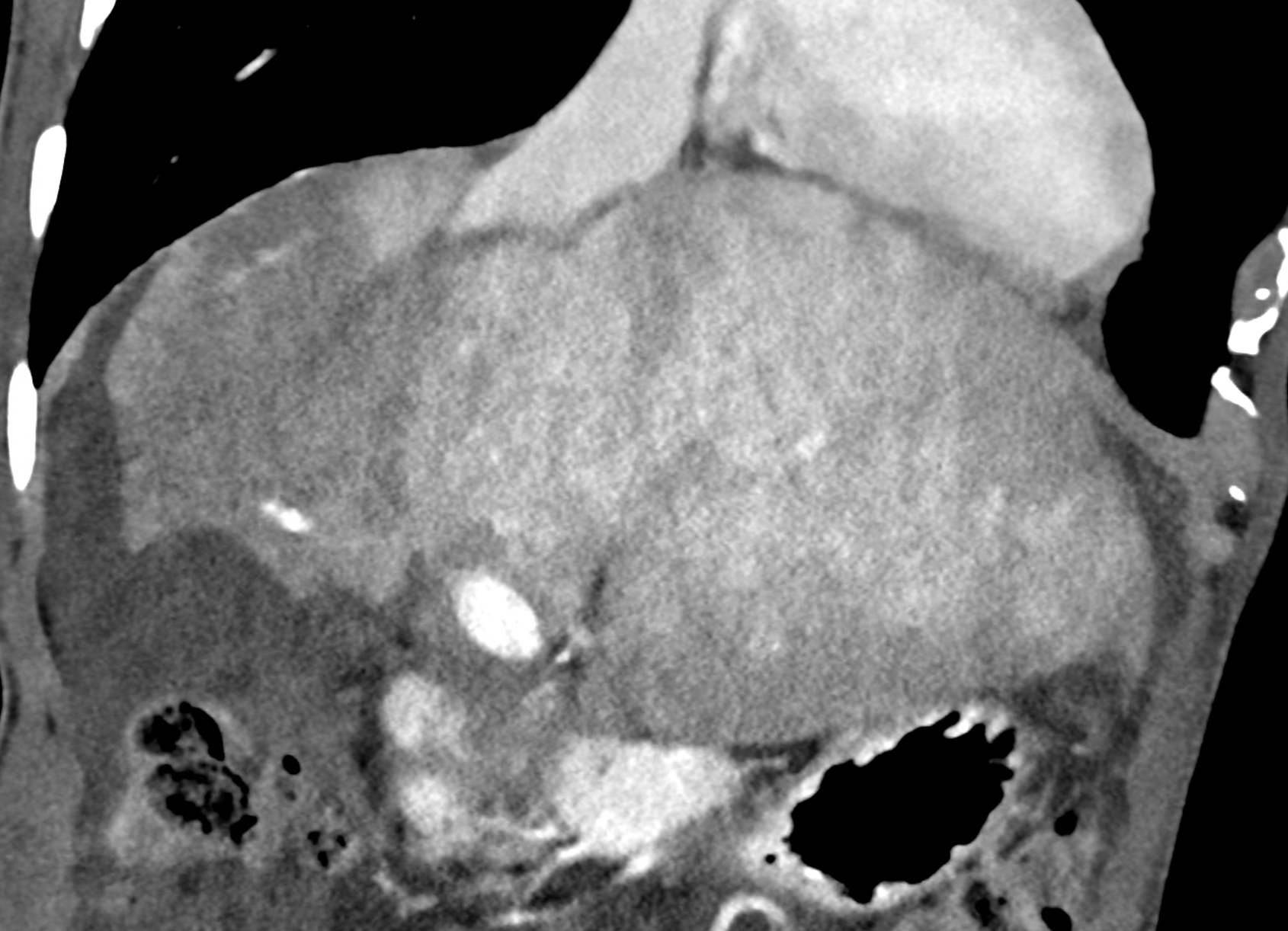
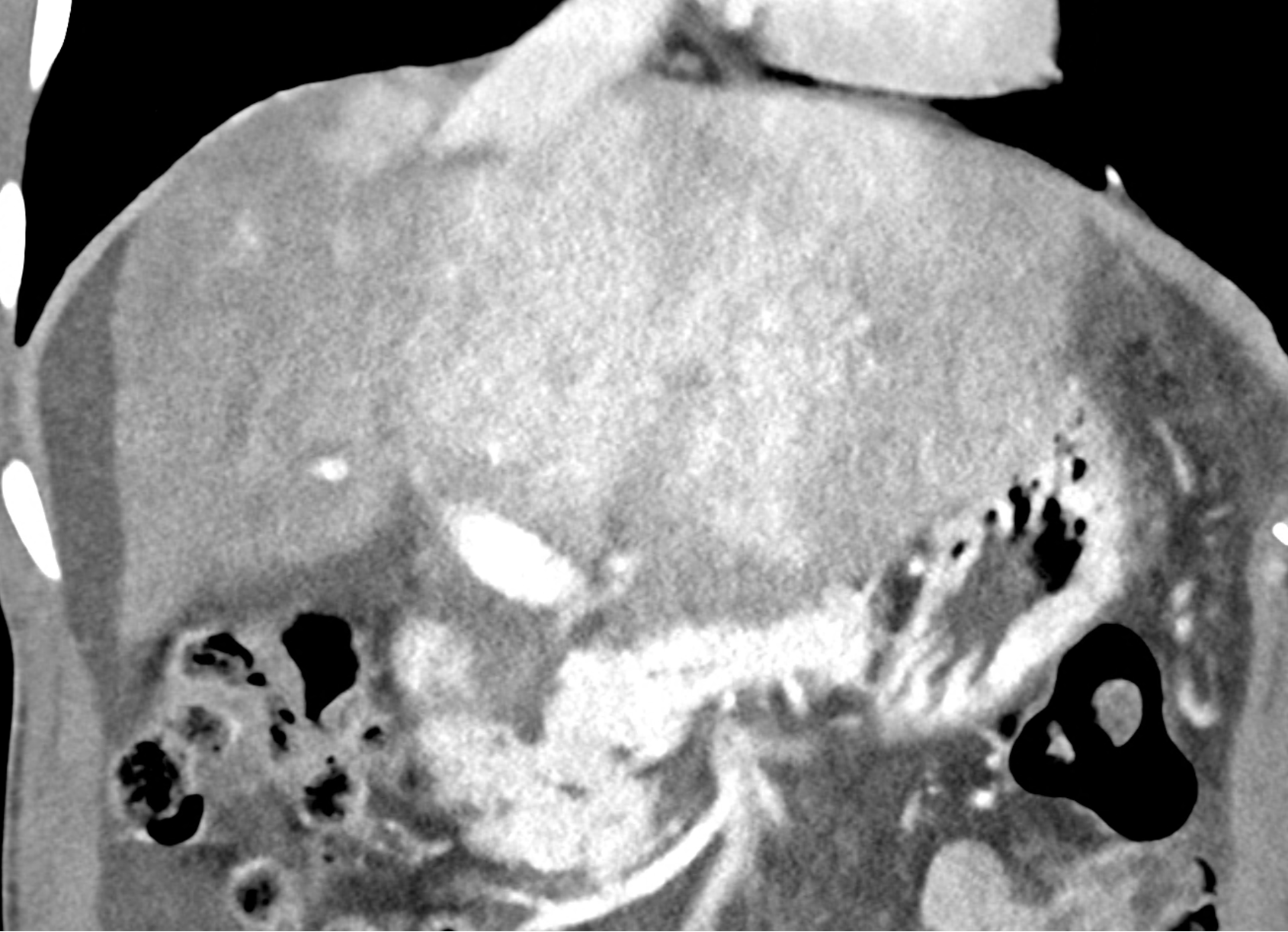
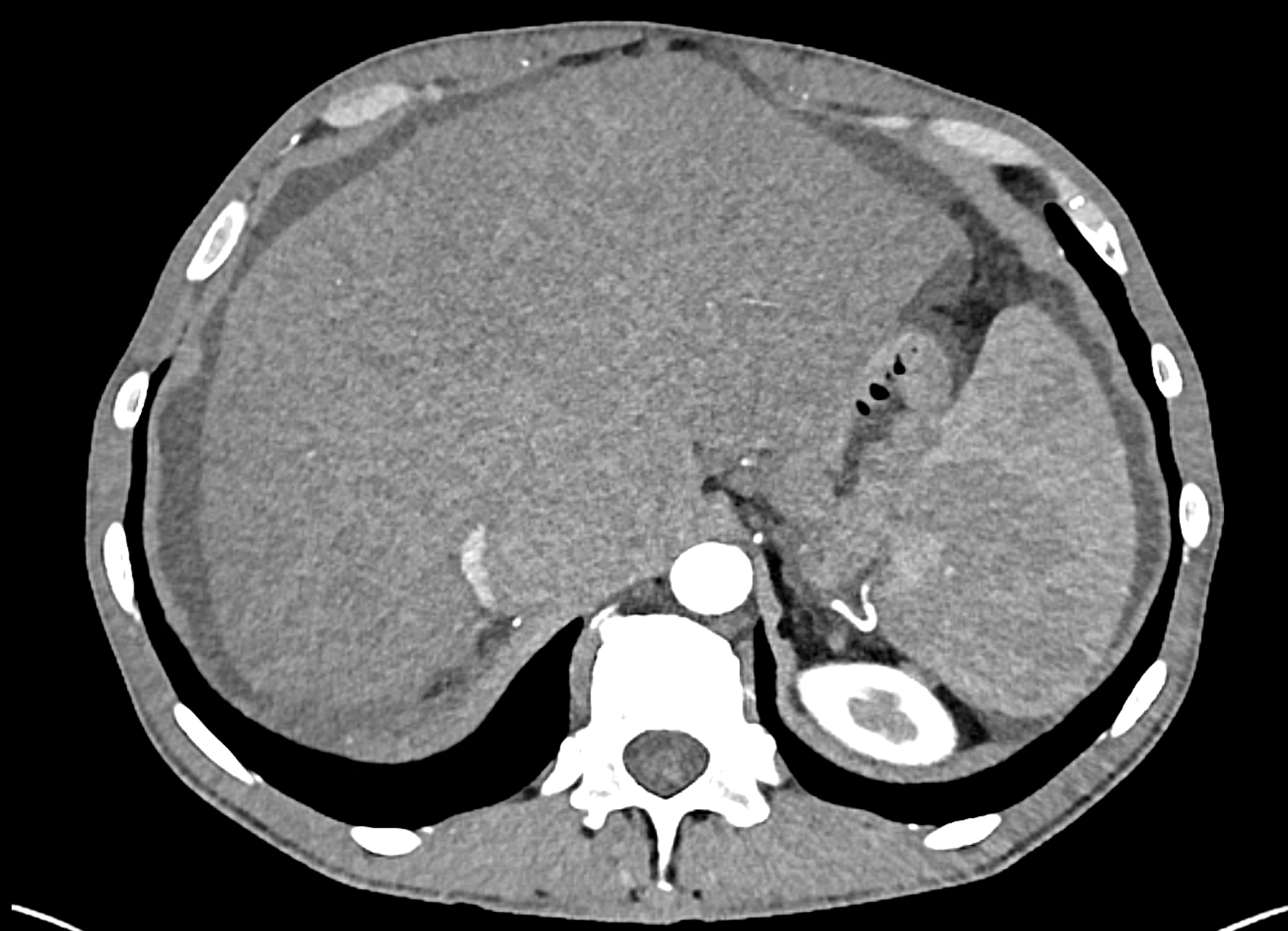
the axial images in the arterial, and the portal phases


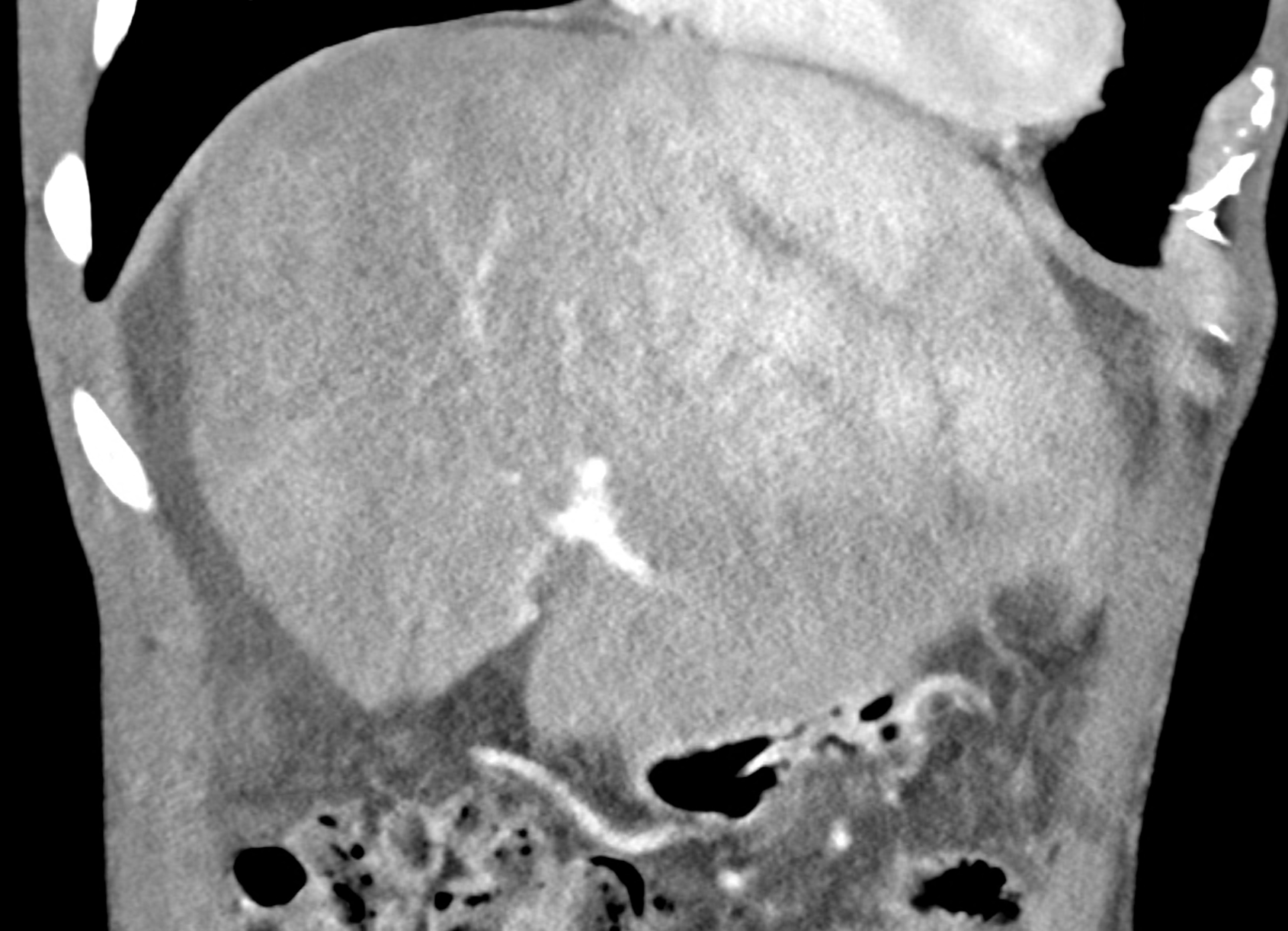
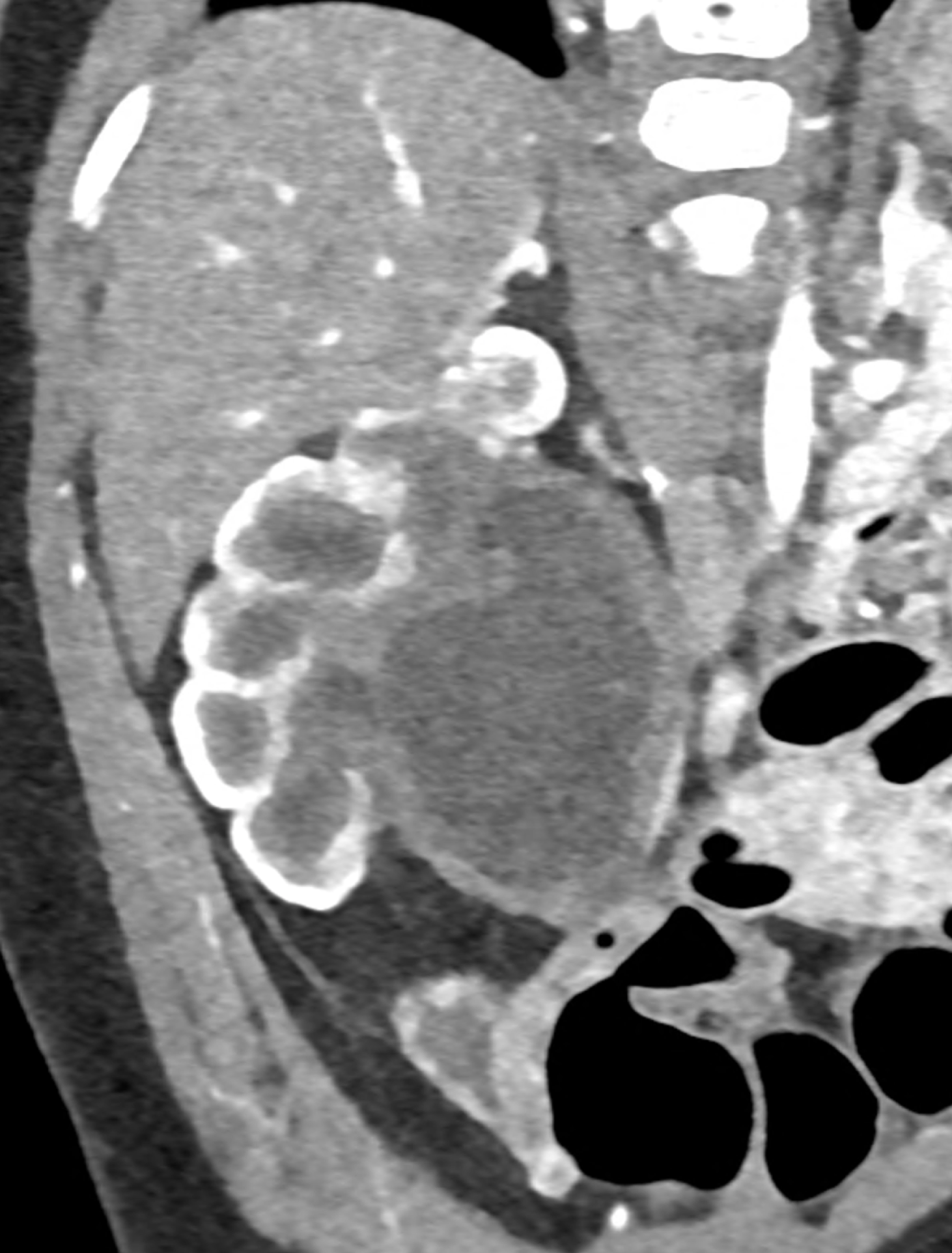
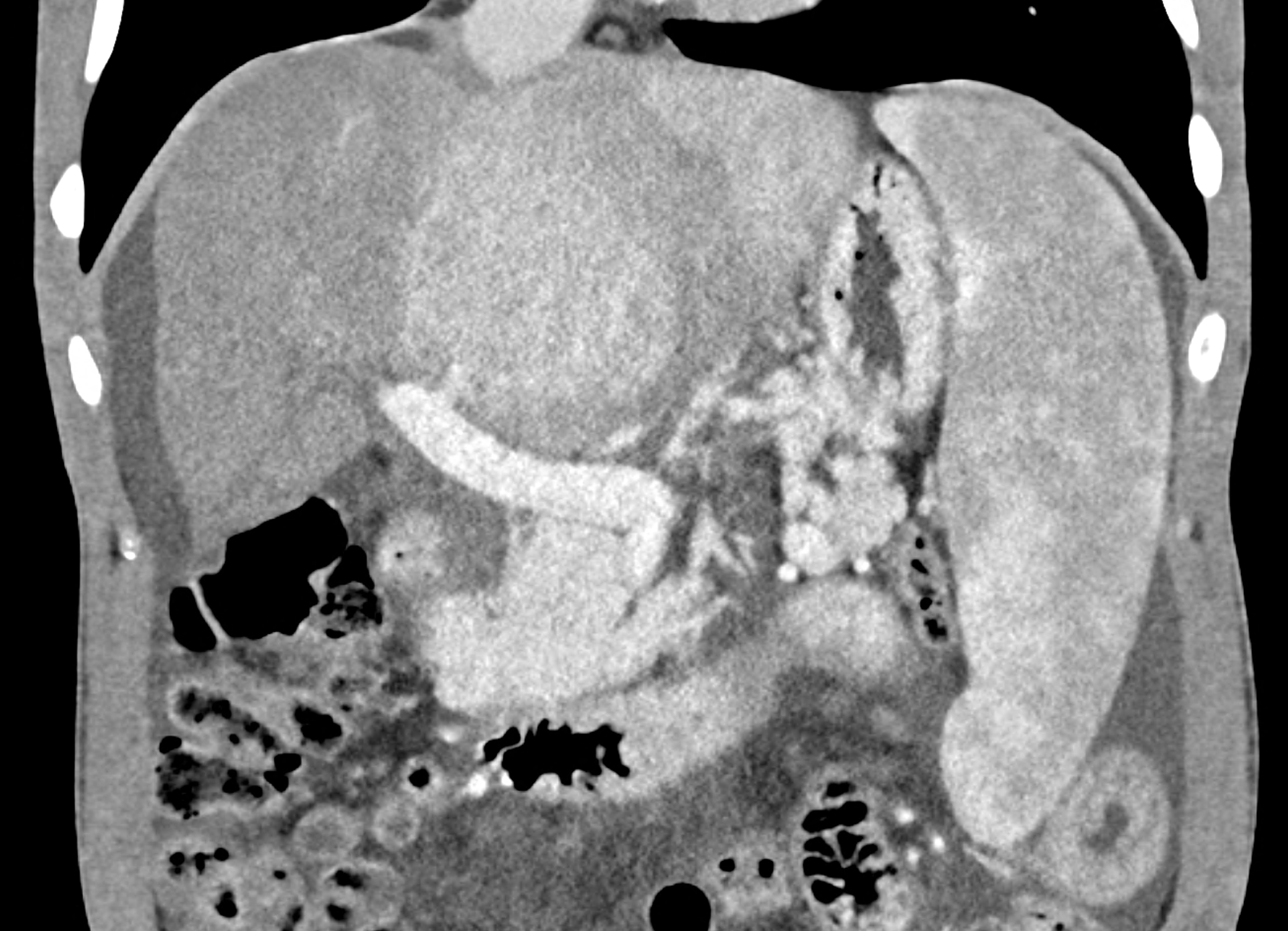
coronary view documenting splenomegaly, different enhancement of the liver parenchyma, and ascites, the arterial, and the portal phases
multiplanar reconstructions showing occluded radices of hepatic veins