

Intramural hematoma is a pathological condition classified as an acute aortic syndrome, in which a hematoma forms in the tunica media. Aortic intramural hematoma (IMH) is the result of bleeding from a rupture of the vasa vasorum or from the penetration of an arteriosclerotic ulcer, provided that there is no complete separation of the tunica intima and the formation of a false lumen in which blood flows. The expansive behavior of IMH itself is similar to the expansion of a false lumen of the aortic direction, but there is no filling with contrast medium. The main factors leading to the development of IMH are hypertension and atherosclerosis. The development of IMH can be its spontaneous regression, progression of the expansive behavior of the hematoma, rupture of the aorta with the development of mediastinal hemorrhage, or transformation into a classic dissection with all its possible complications. As with dissection, IMH is classified according to the Stanford scheme into type A affecting the ascending aorta and type B, where the ascending aorta is spared. In type A, intrapericardial rupture communicating with the aortic recess of the pericardial sac may also occur. CT signs of iIMH are crescent-shaped wall thickening showing the density of coagulated blood, which can be demonstrated using photon-counting CT with virtual native imaging or spectral imaging with monoenergetic images at a higher energy of 140-190 keV. To reduce motion artifacts and visualize the coronary arteries, it is also advisable to use ECG-synchronized data acquisition.
case report
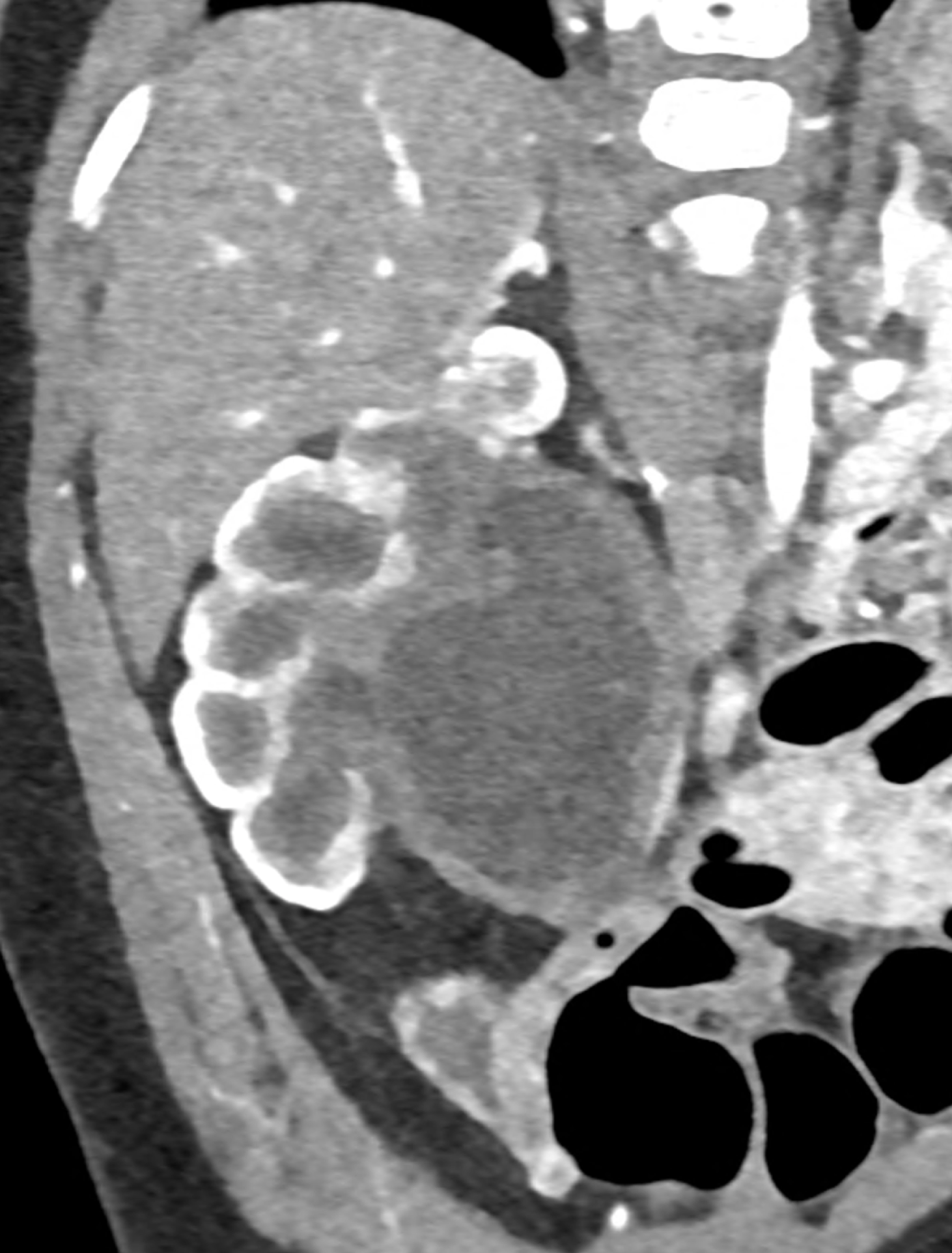
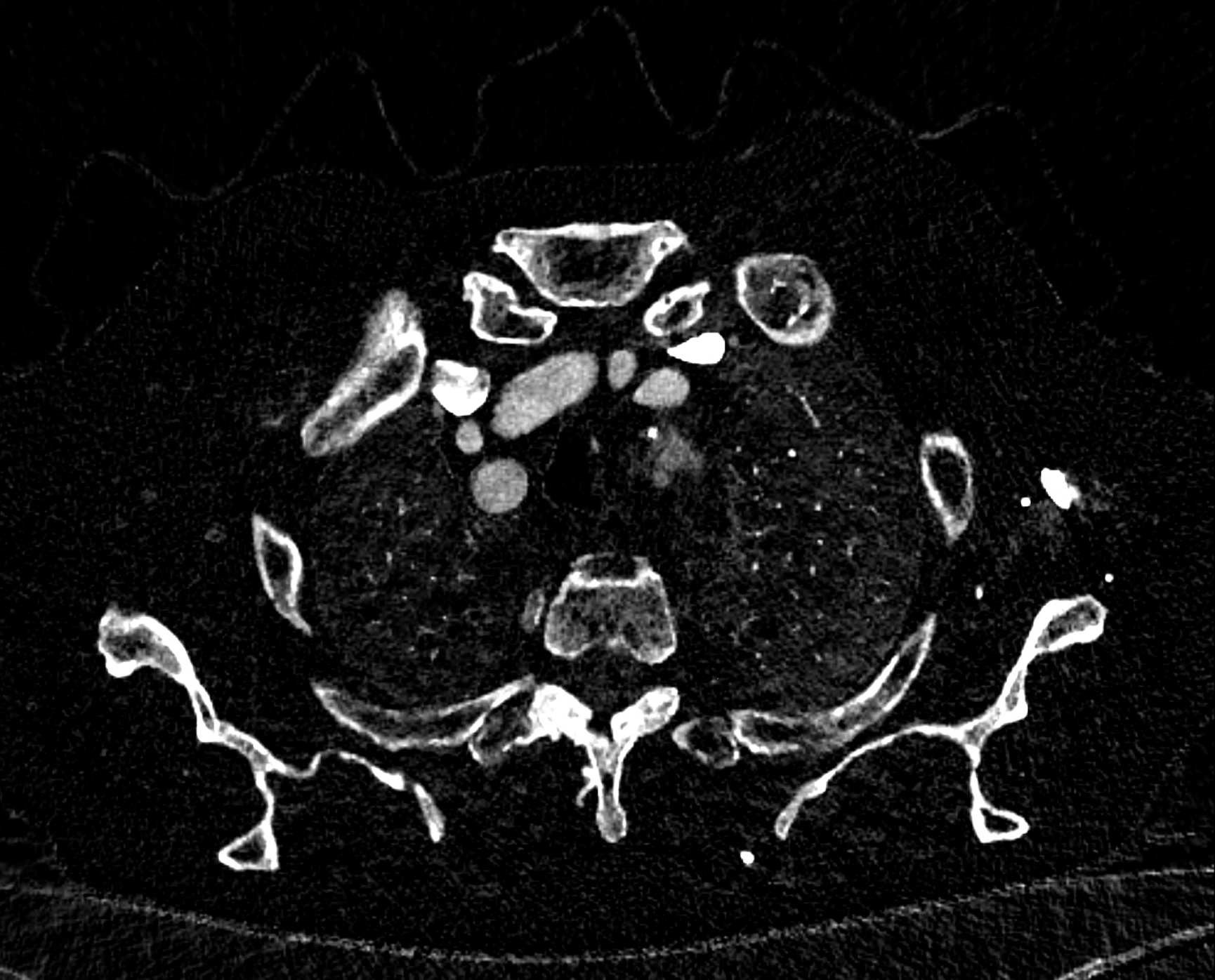
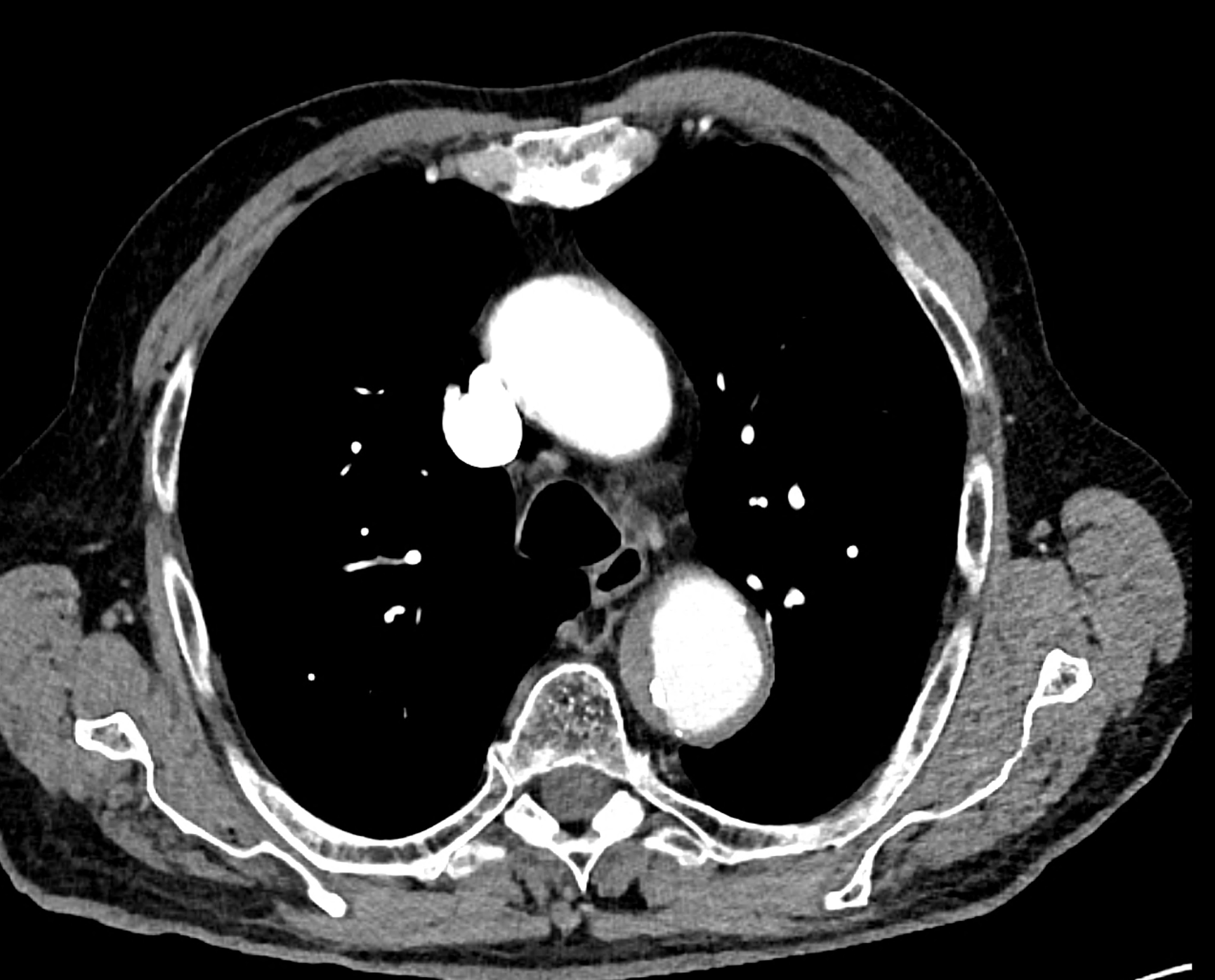
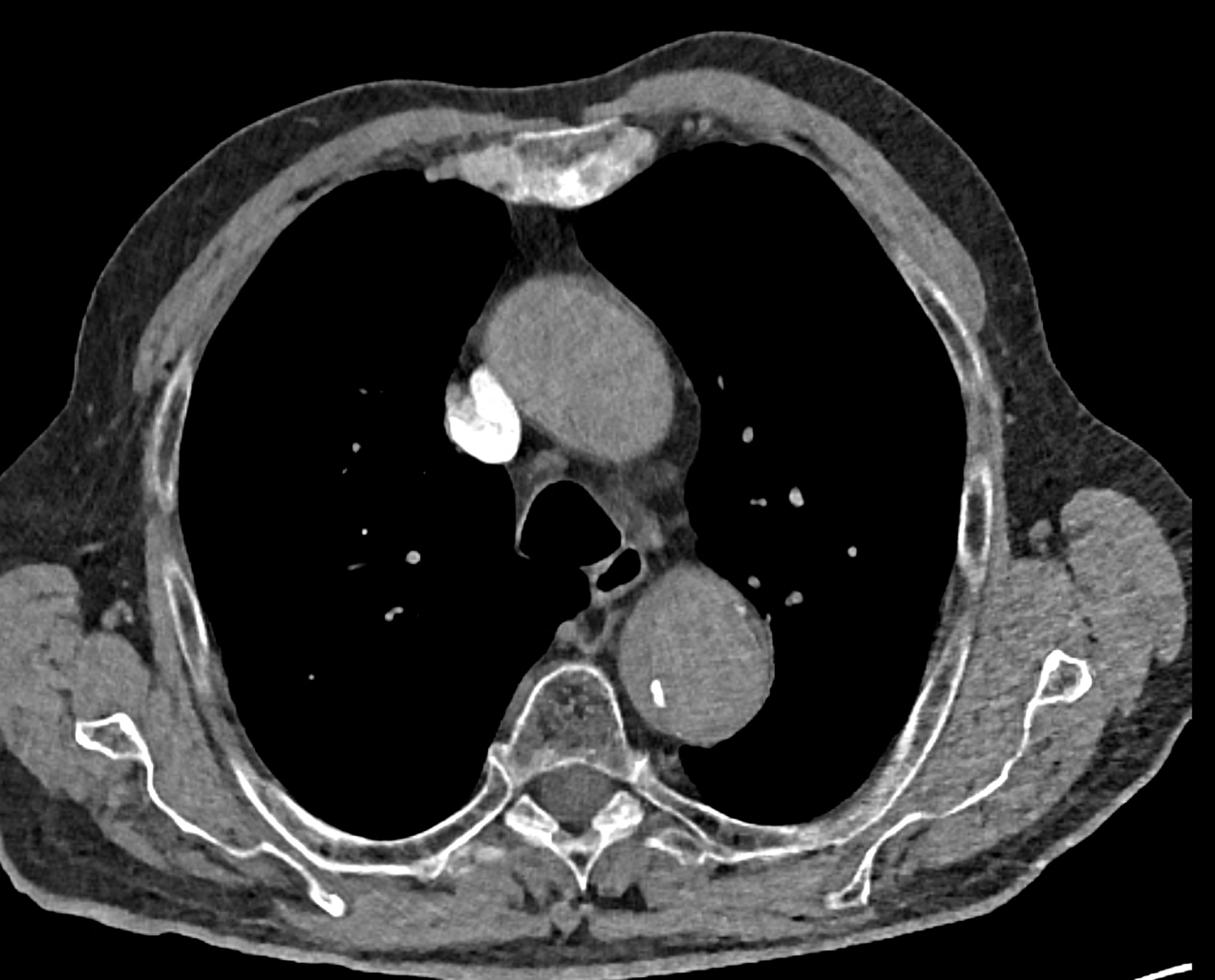
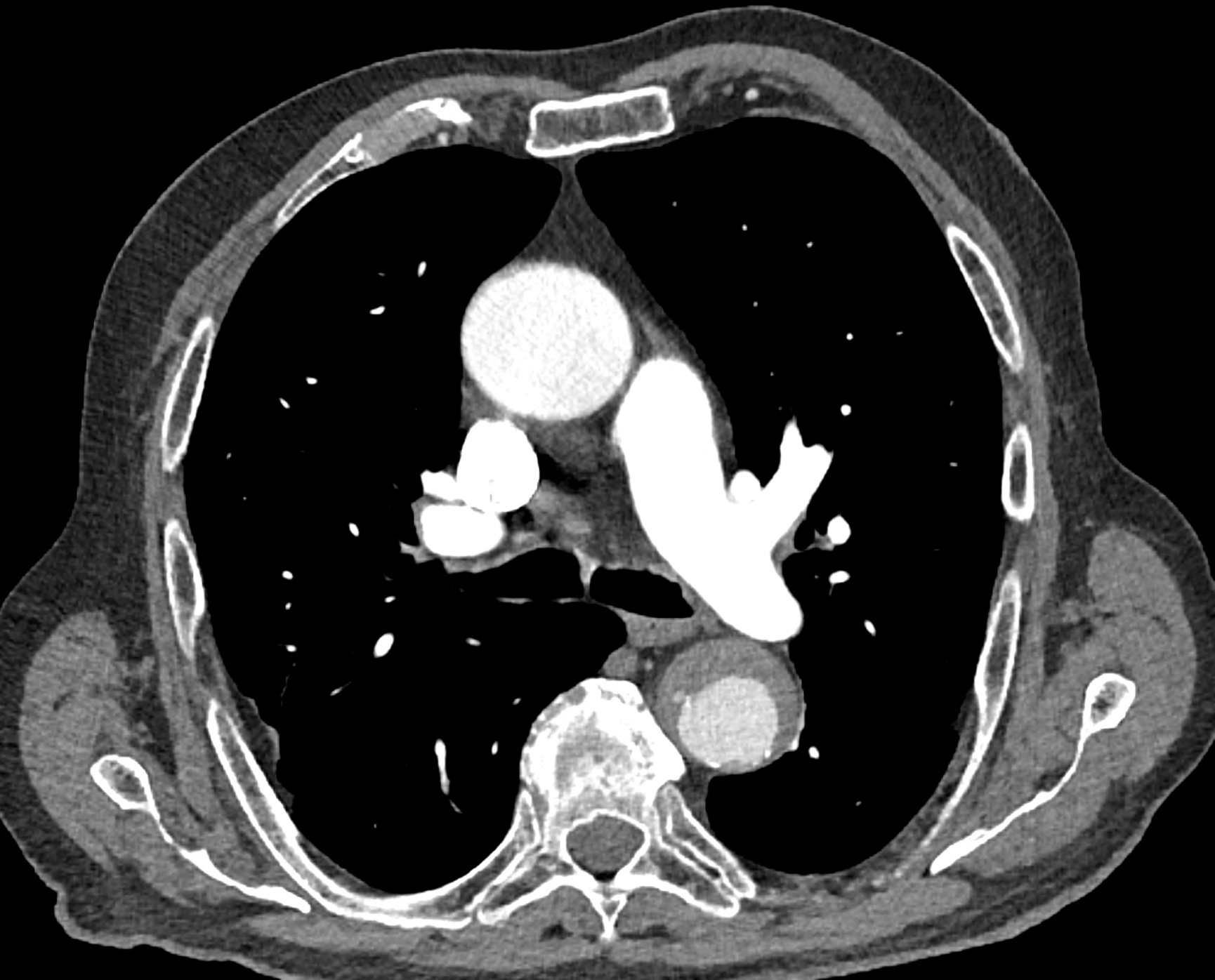
in patient chest pain, negative ECG but with elevated D-dimers was performed CTA of the chest to exclude highly suspected pulmonary embolism. No pulmonary embolism was see, but the pathology of the aortic arch and descending thoracic atorta. The images were consistent with aortic intramural hematoma type B according to the Stanford classification with incipient transformation in dissection – behind the subclavian artery, it is clear that the contrast agent is flowing into the intramural hematoma. Differentiation from wall thrombosis is facilitated by the presence of calcification in the detached intima, which is most clearly visible on virtual non-contrast imaging. The intramural hematoma itself exhibits different properties in terms of X-ray absorption. Coagulated blood is visible at the apex of the aortic arch, where it closely adjoins the area that is perfused and filled with contrast medium. There are other smaller areas filled with contrast medium at the sites of the intercostal arteries. These areas are secondary sites where the original intramural hematoma is channeled during its transformation into a classic aortic dissection.
Virtual non-contrast images help to distinguish between the intima and thus in the differential diagnosis of intramural hematoma versus wall thrombosis. Signs of fresh coagulated blood in IMH indicate bleeding into the aortic wall from the vasa vasorum. In contrast, monoenergetic images with lower energies of 40-55 keV highlight areas of intramural hematoma with active blood flow.
Naeotom Alpha.Peak, University Hospital Pilsen, Czechia
comparison of the the images 60, keV monoenergetic, virtual non-contrast (VNC), and iodine map images. The repercussion starts in the proximal tear of the intimate (the first three images), calcification in the intimate (next three images), tera at the level of the arising intercostal artery (last three images)





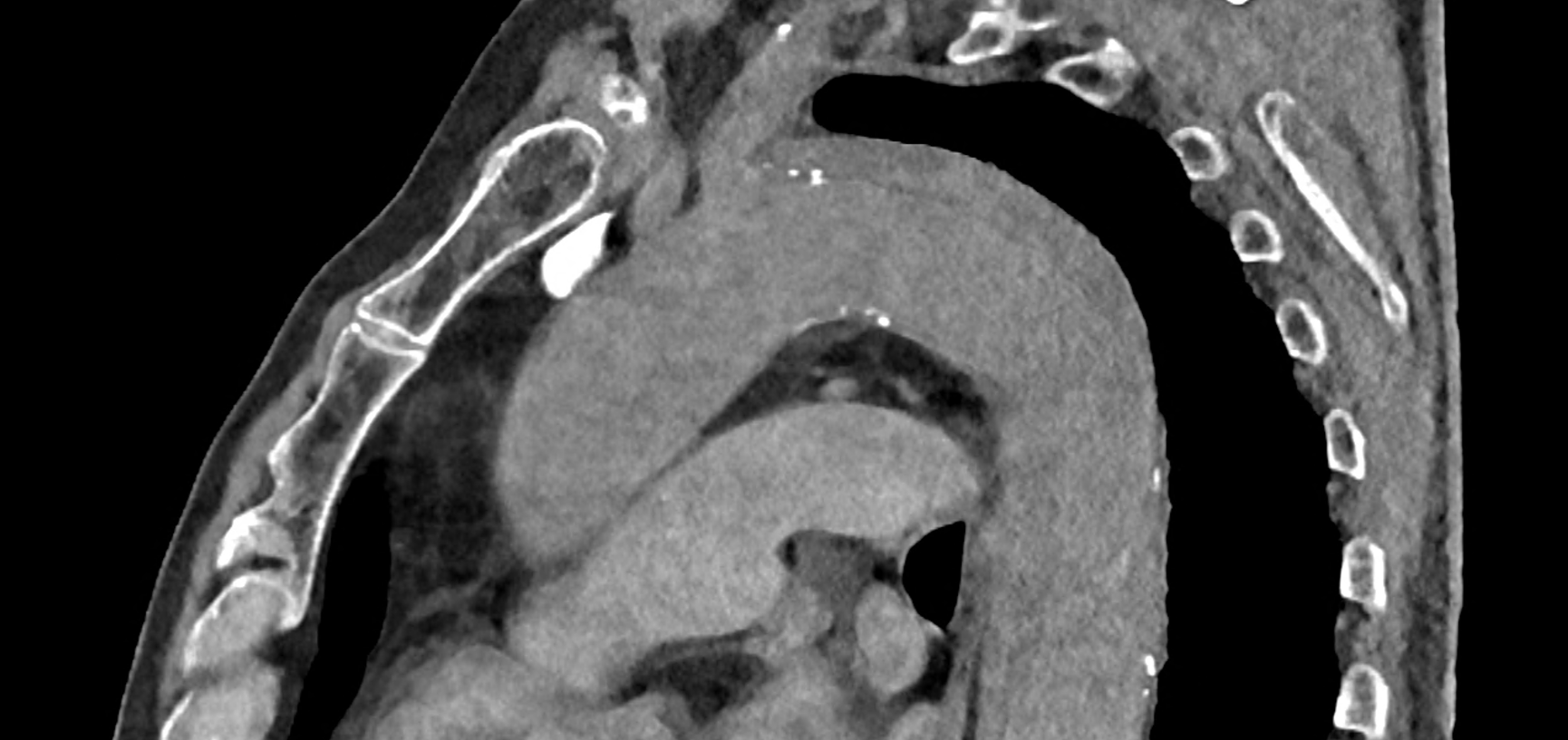
comparison of the sagittal aortic MPR in 40, 60, 140 and 190 keV monoenergetic images




comparison of the perpendicular planes to sagittal aortic MPR in 40, 60, 140 and 190 keV monoenergetic images



