

splenic rupture
Spleen injury occurs in blunt abdominal trauma, when the force is concentrated in the upper left abdominal quadrant, or in combination with fractures of the causal ribs on the left side of the chest, typically with fractures of ribs 9-11. The long axis of the spleen runs parallel to the 10th rib on the left.
The continuity of the spleen is interrupted when it is torn (lacerated), and the tear is hypodense, filled with hypodense blood. Spleen injury is more clearly visible in the later phase of saturation, i.e., in the portal phase after the administration of iodine contrast medium. In the earlier phase, it is necessary to pay attention to the different saturation of the red and white pulp. The significance of bleeding is assessed both in terms of bleeding activity and in terms of the volume of hemoperitoneum. In the CT image, a sign of rapid bleeding is the leakage of contrast medium from the vascular lumen with accumulation around the injured vessel. Active bleeding associated with the leakage of contrast medium outside the vascular space can be demonstrated by spectral analysis using photon-counting CT with virtual non-contrast imaging (VNC) or iodine distribution mapping
dual-phase rupture of the spleen
dual-phase rupture of the spleen occurs during blunt trauma to the abdomen in a situation where the renal capsule, i.e., the peritoneal surface of the spleen, is not initially damaged, but only a tear inside the parenchyma. A collection of blood in the form of a subcapsular hematoma, which has a seminal shape, is often found under the papule. The tear inside the parenchyma may not be completely visible. Subsequent bleeding into the enclosed space creates excess pressure, which then causes the spleen capsule to rupture when the resistance is exceeded. The rupture of the capsule then releases the pressure and accelerates the bleeding, resulting in hemoperitoneum. Due to the high blood flow through the spleen, bleeding can be relatively rapid, resulting in more pronounced hemoperitoneum in the subphrenic left space around the spleen, but also in the right space around the liver and in the pelvic excavation of the Douglas’ space.
In CT imaging, a sign of rapid bleeding is the leakage of contrast medium from the vascular lumen with accumulation around the injured vessel. Active bleeding can be detected by spectral analysis using photon-counting CT with virtual non-contrast imaging (VNC) or iodine distribution mapping.
case report
Spleen injury after a fall from a bicycle, when an ultrasound examination initially revealed a small subcapsular hematoma of the spleen. A CT scan confirmed the finding without revealing any major injury to the spleen itself. A conservative approach was taken, with the patient being monitored clinically in the surgical ward. After 24 hours, the findings were completely stable, as confirmed by a follow-up ultrasound examination, clinical examination, and blood count. Forty-eight hours after the injury, the patient suddenly developed pain in the left half of the abdomen, tachycardia, and a sudden drop in blood count. A CT scan revealed a large hemoperitoneum with contrast agent leaking from the lacerated spleen. CT angiography clearly shows contrast agent leaking from the injured vessel. The virtual native image then shows coagulated blood around the spleen and also directly at the site of the tear in the spleen parenchyma.
Naeotom Alpha.Peak, University Hospital Pilsen, Czechia
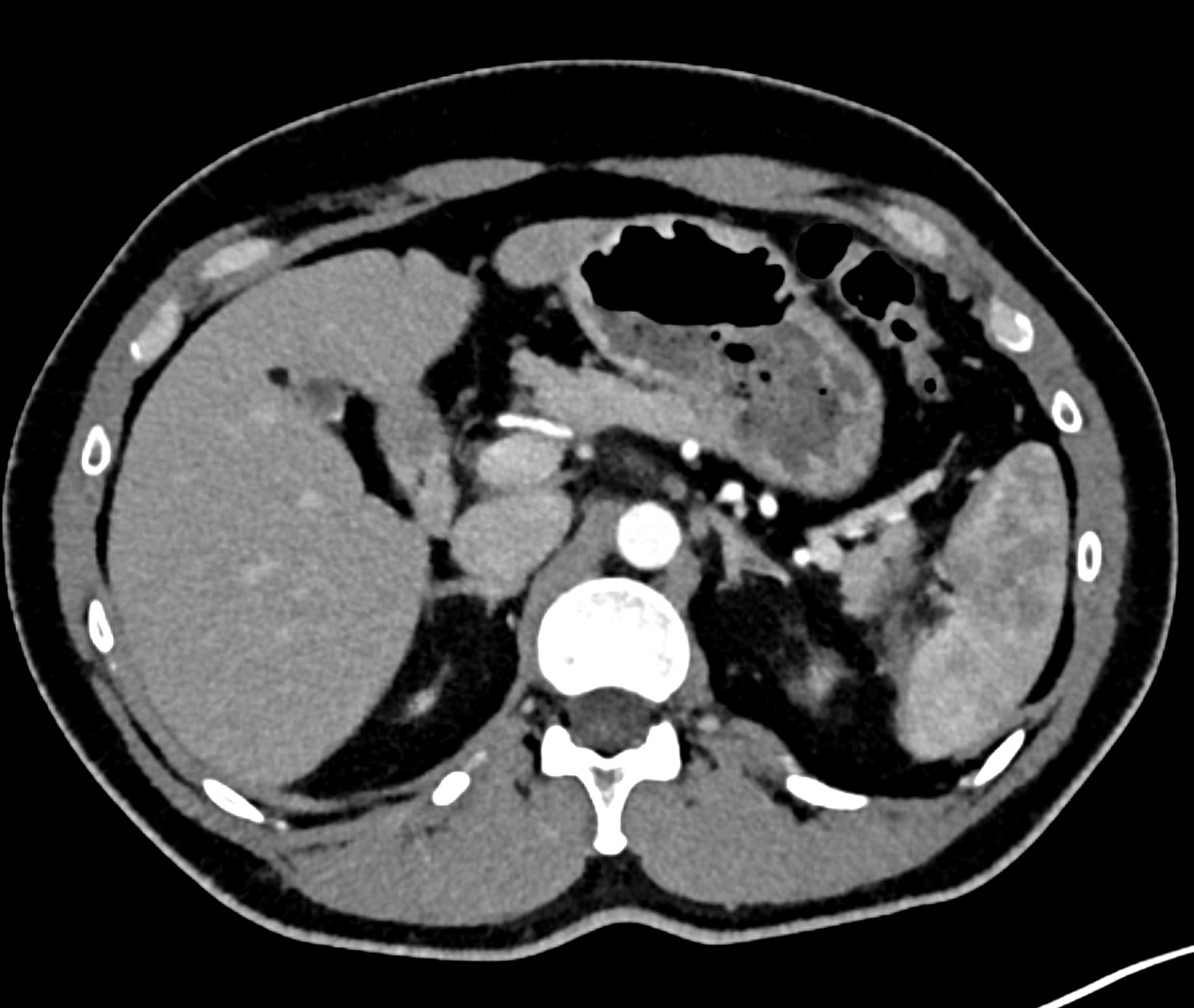
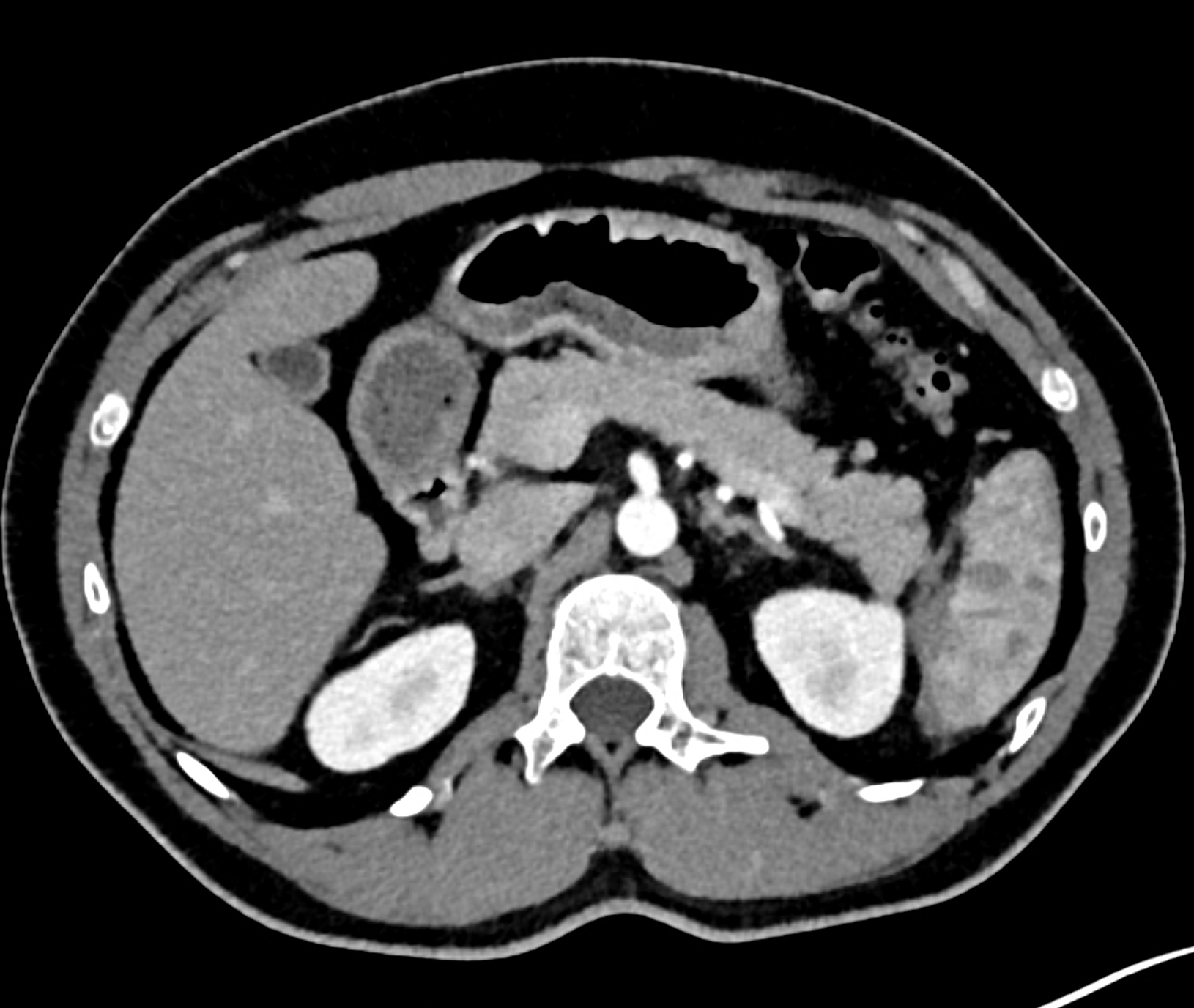
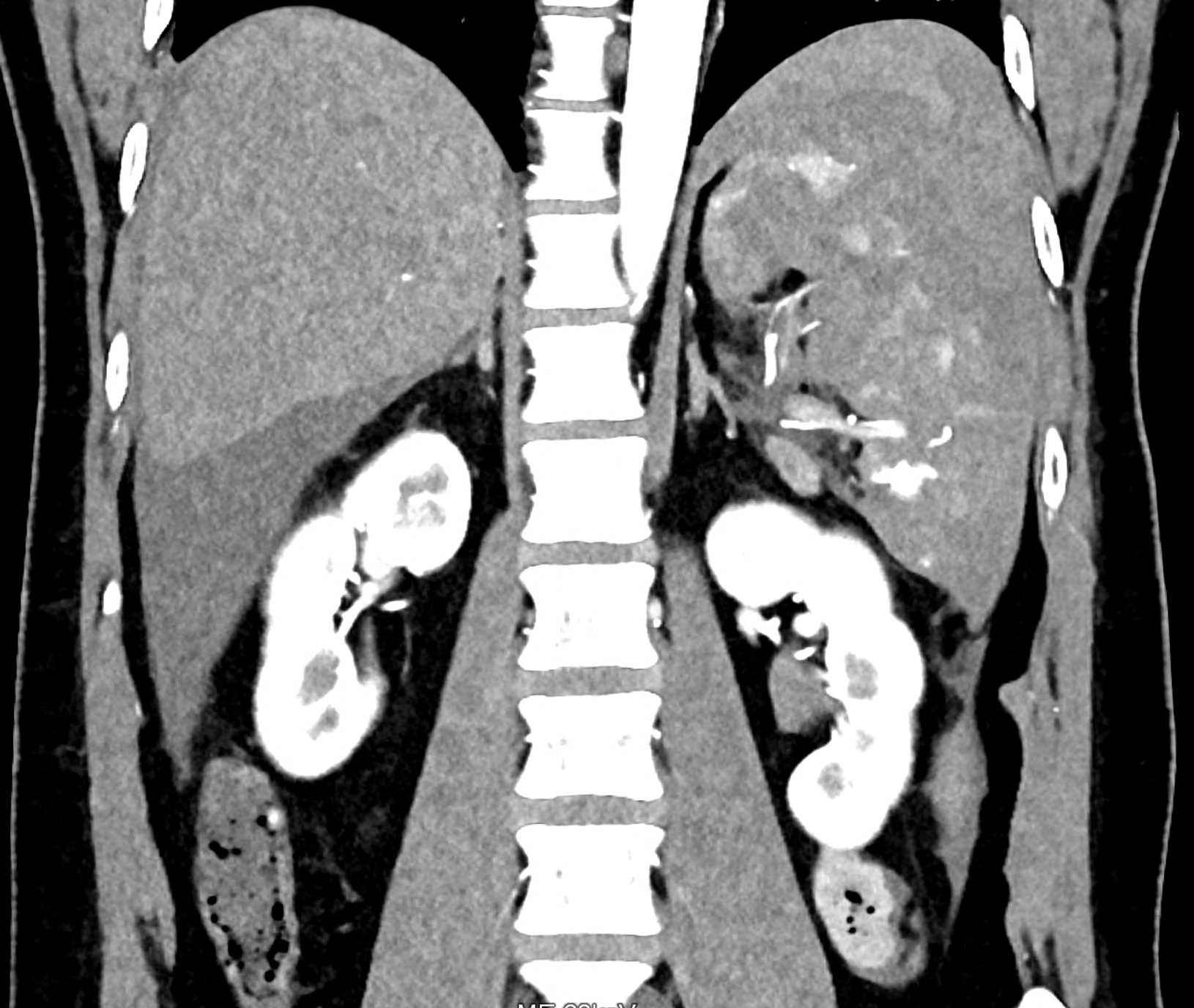
CT images 90 minutes after the fall from bicycle in the arterial phase showing sub capsular hematoma and the tear in the lower third of the spleen

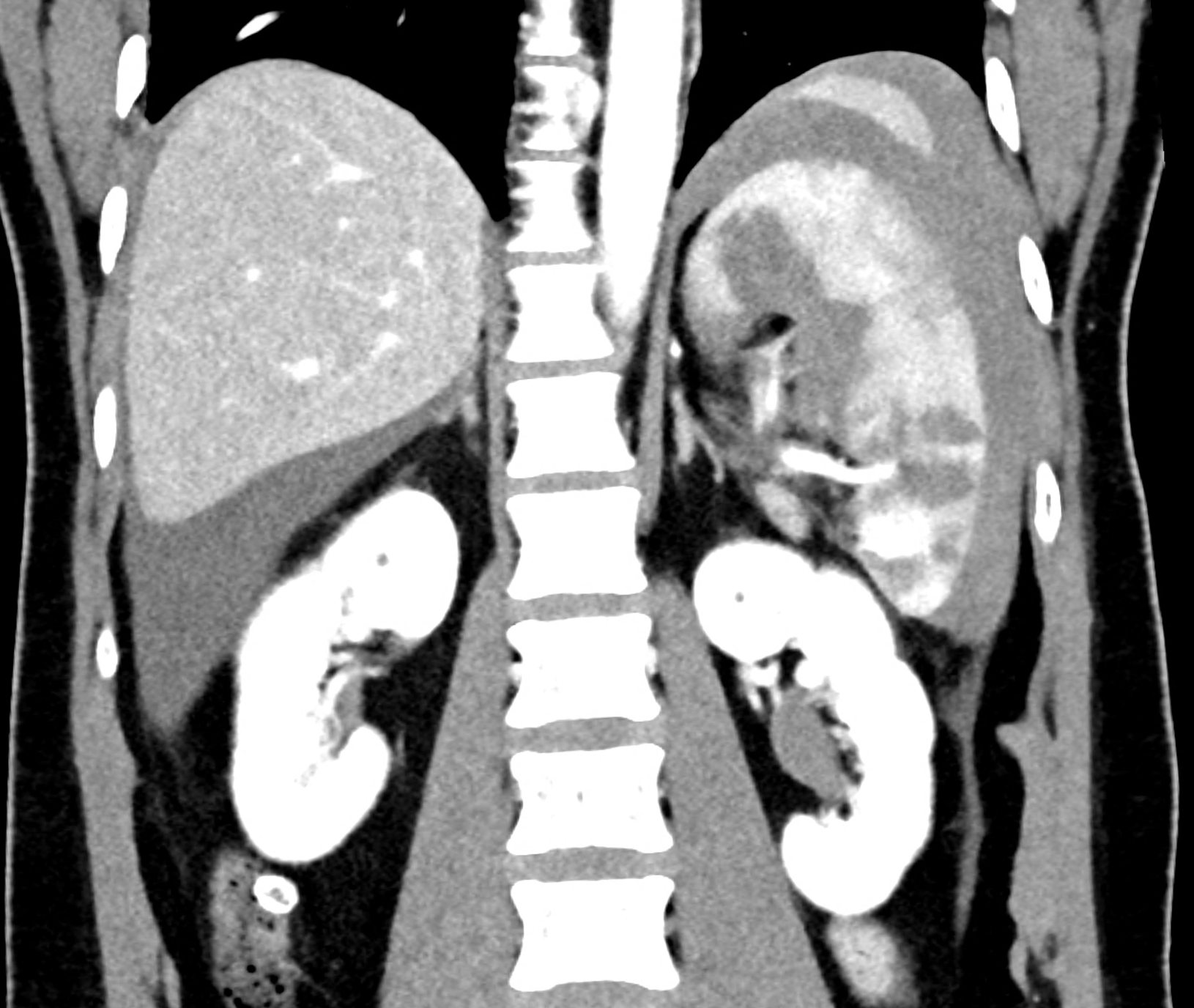
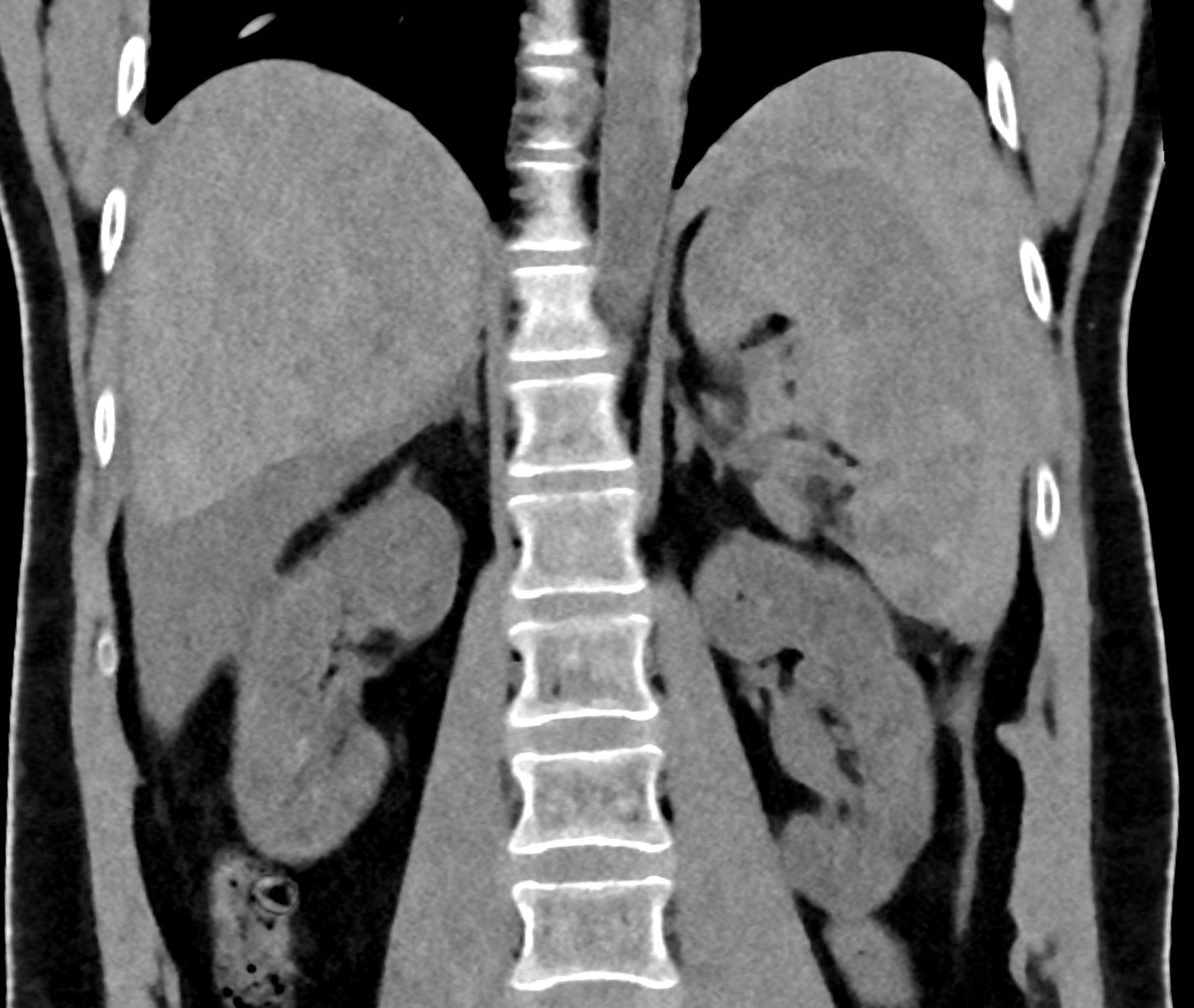
follow-up study 48 hours later during worsening of the patient’s state
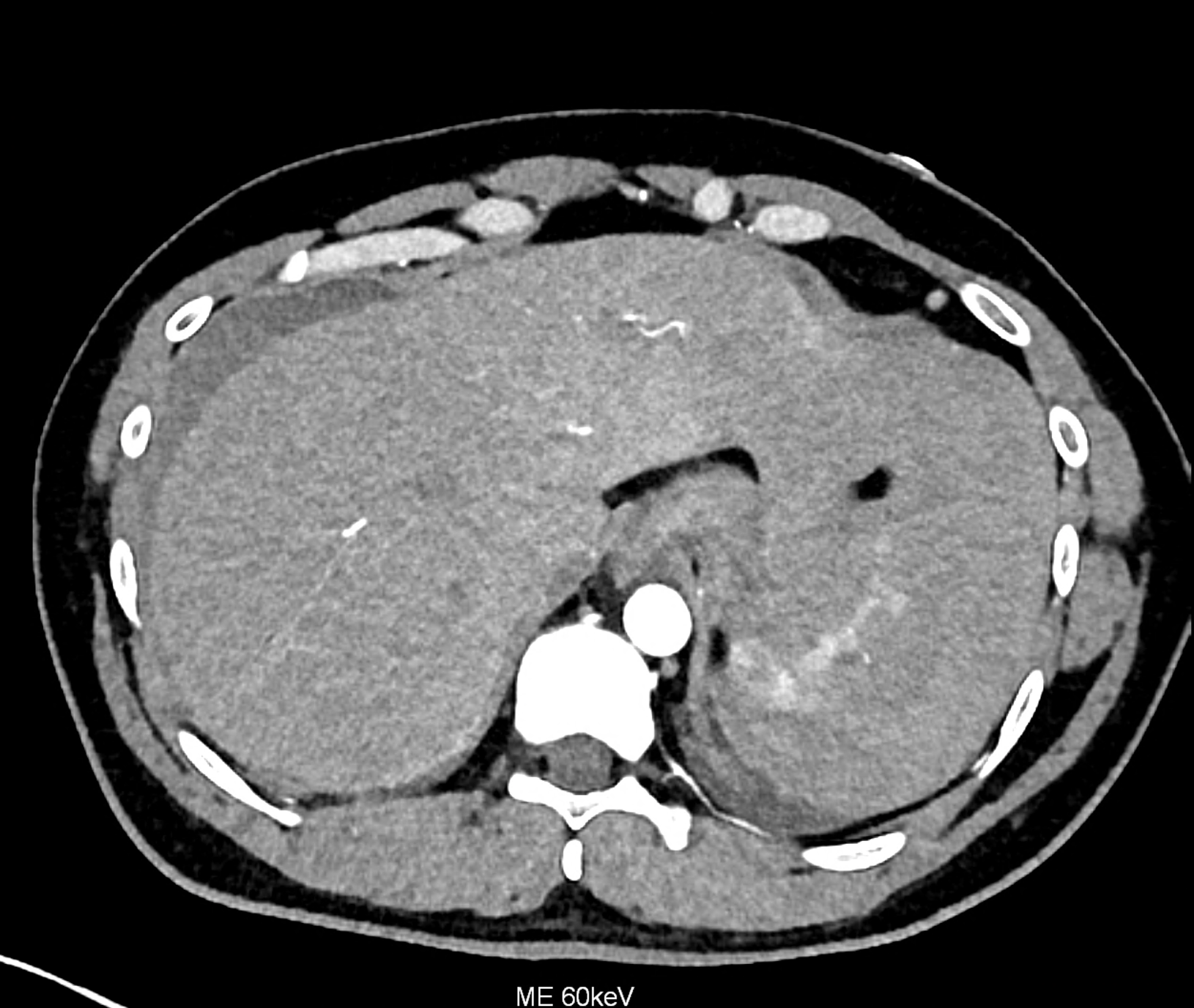
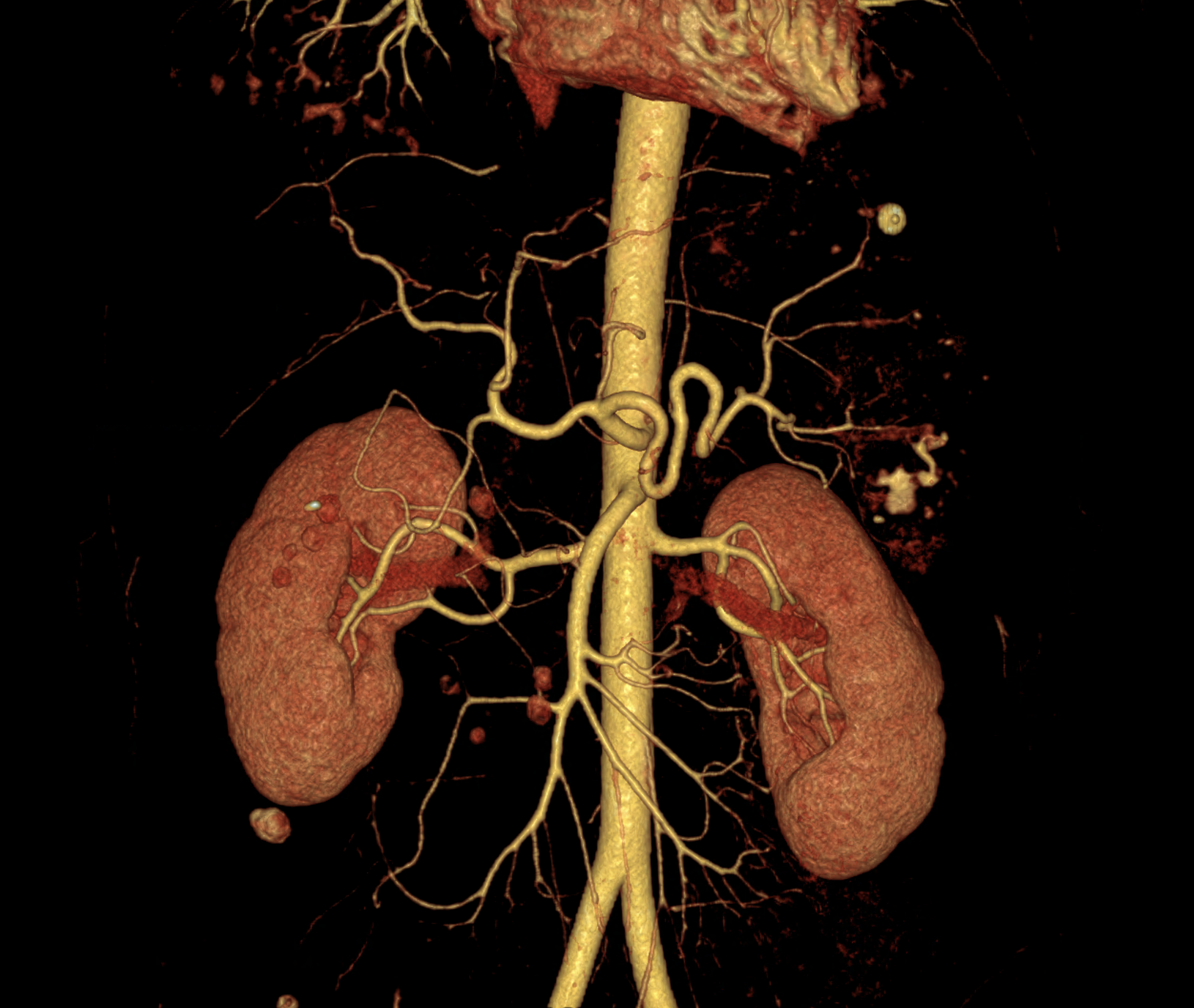
CT angiography showing the leakage of ht contract agent in the lower third of the spleen
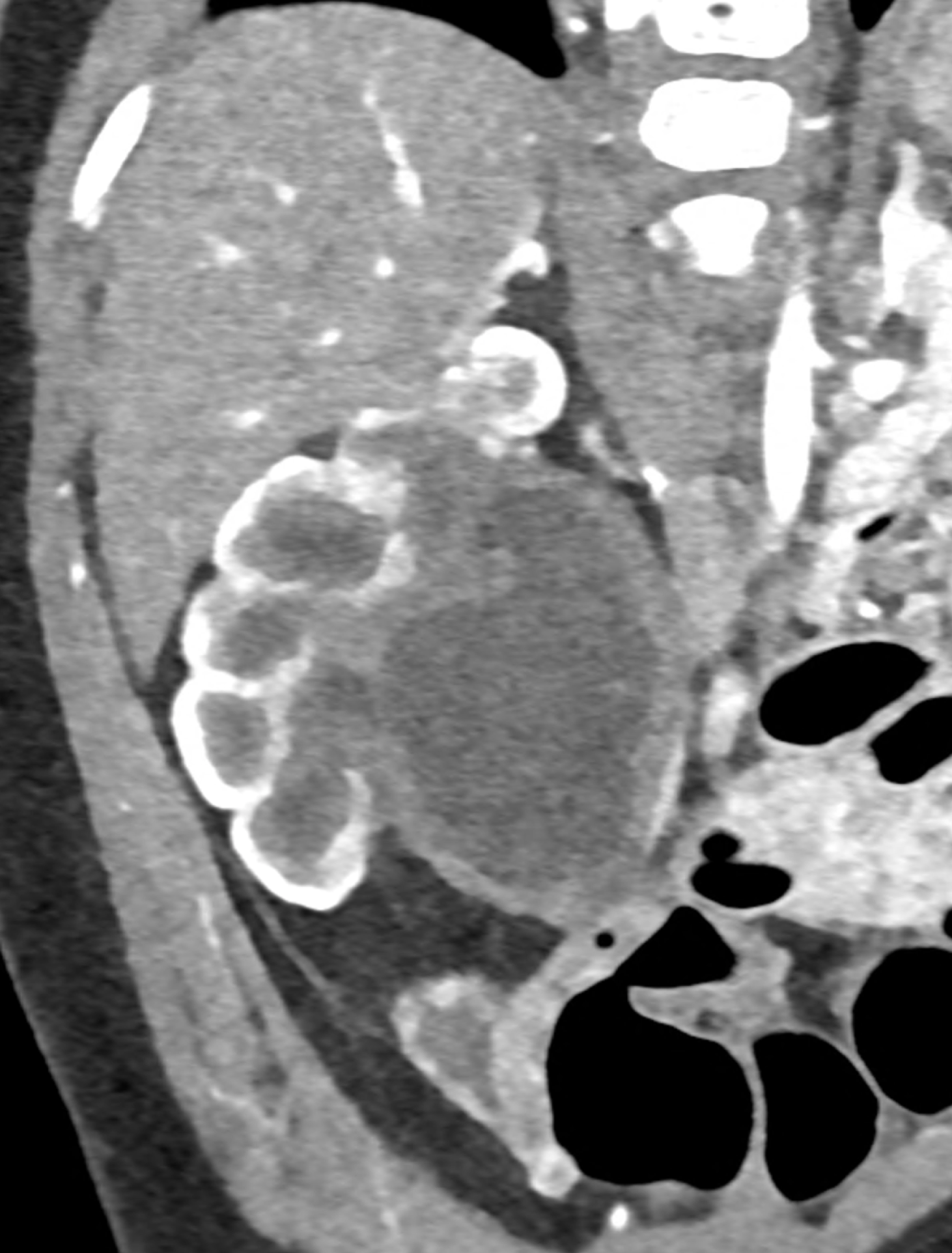
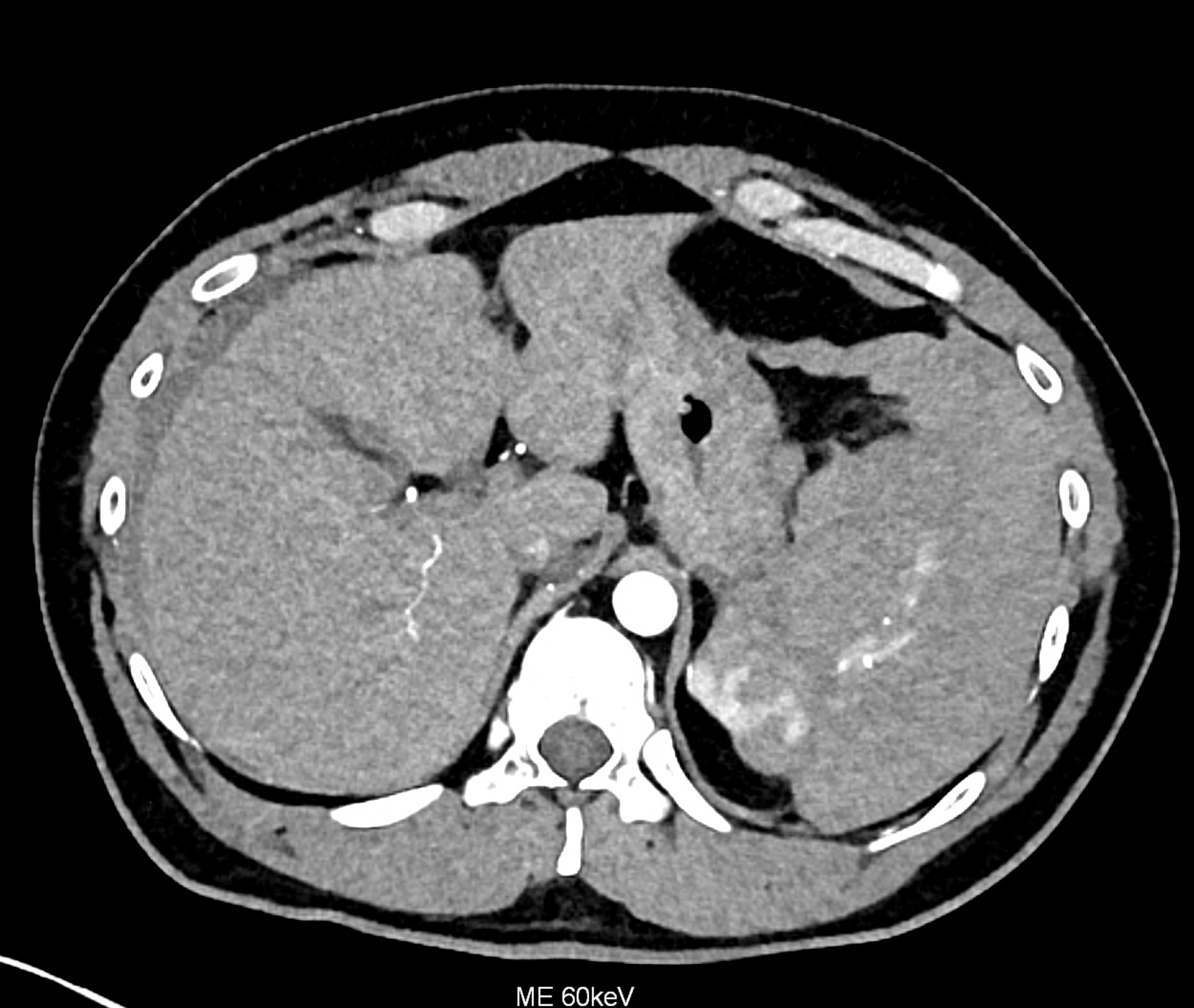
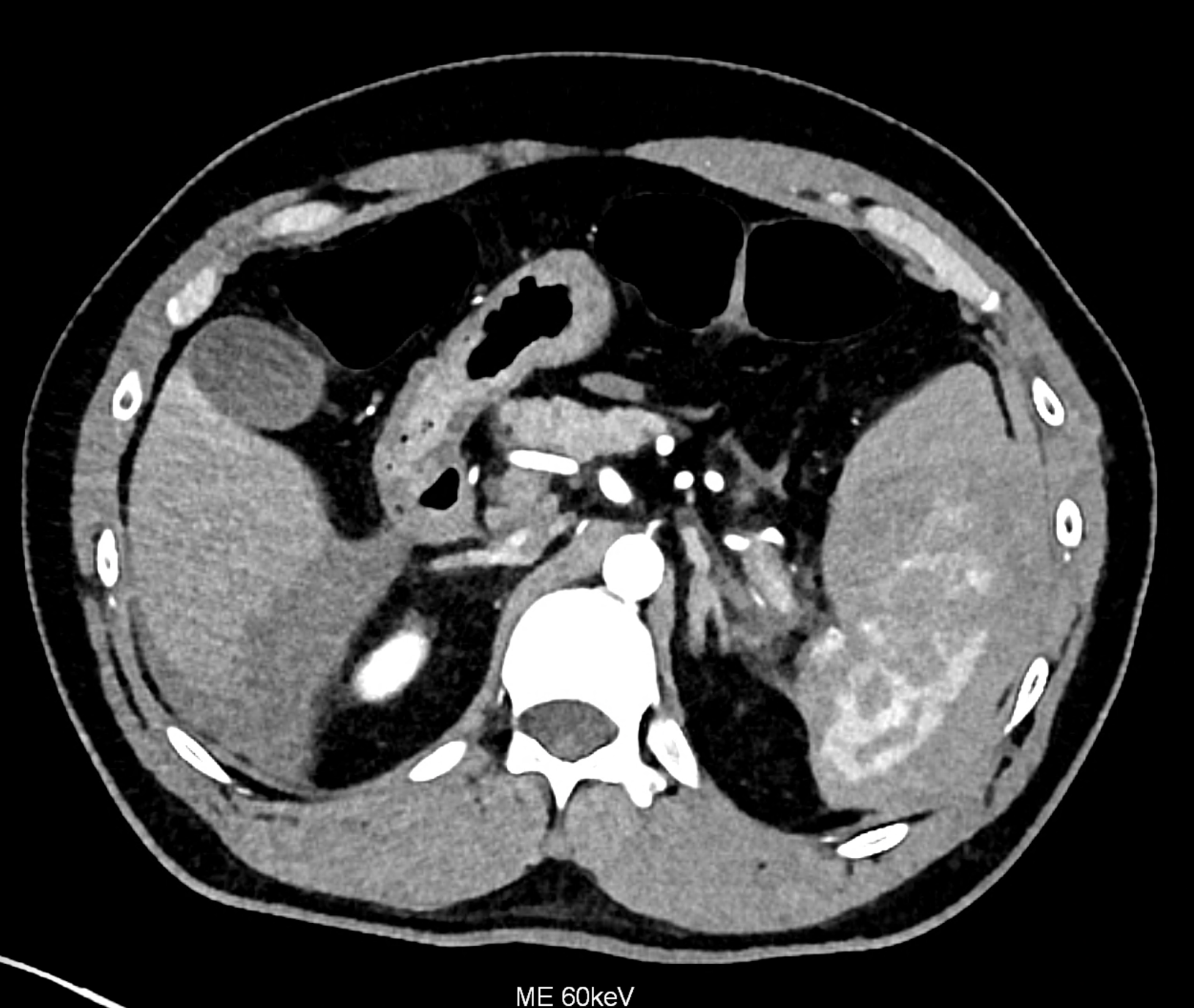
comparison of the monoenergetic images in 60 keV and virtual non-contrast (VNC) in portal phase of iodinated contrast distribution in the coronary and the axial planes


Leave a Reply