technique of CT enterography
CT enterography data acquisition follows after oral preparation of the small intestine by fractionated sipping of 2-5% aqueous mannitol solution. Fractional sipping a contrast agent in doses of 50 – 100 ml approximately every two minutes in total amount of 1500 – 2000 ml fills sufficiently entire small and large bowel. The mannitol solution is an isoidense substance with water and it has osmotic effects, thus the bowel loops remain distended. The examination is also performed after the application of spasmolytics (N-butylscopolamine – Buscopan). The administration of spasmolytics is important for the distension of the intestinal wall. Intravenous administration of iodine contrast medium is an important part of the imaging, intravenous application 50 ml of iodinated contrast material with the concentration of 350 mgI/ml is sufficient, the injection flow rate is 3 – 4 ml/s. The enhancement of the inflammatory tissue becomes optimal in the early to peak portal phase. The main indication is Crohn’s disease at all stages of the disease. Photon-counting CT improves the spatial resolution with the ability of the imaging of the tiny structures within the bowel wall including the ulcerations, and also the vascular changes of the mesentery. Spectral imaging improve the imaging of the vascularized inflammatory tissue and then the improved detection of the signs of the disease activity. The monoenergetic images in 40 – 55 keV increase the contrast between inflammatory changes, edema and muscular parts of the bowel wall
note of the pathological anatomist
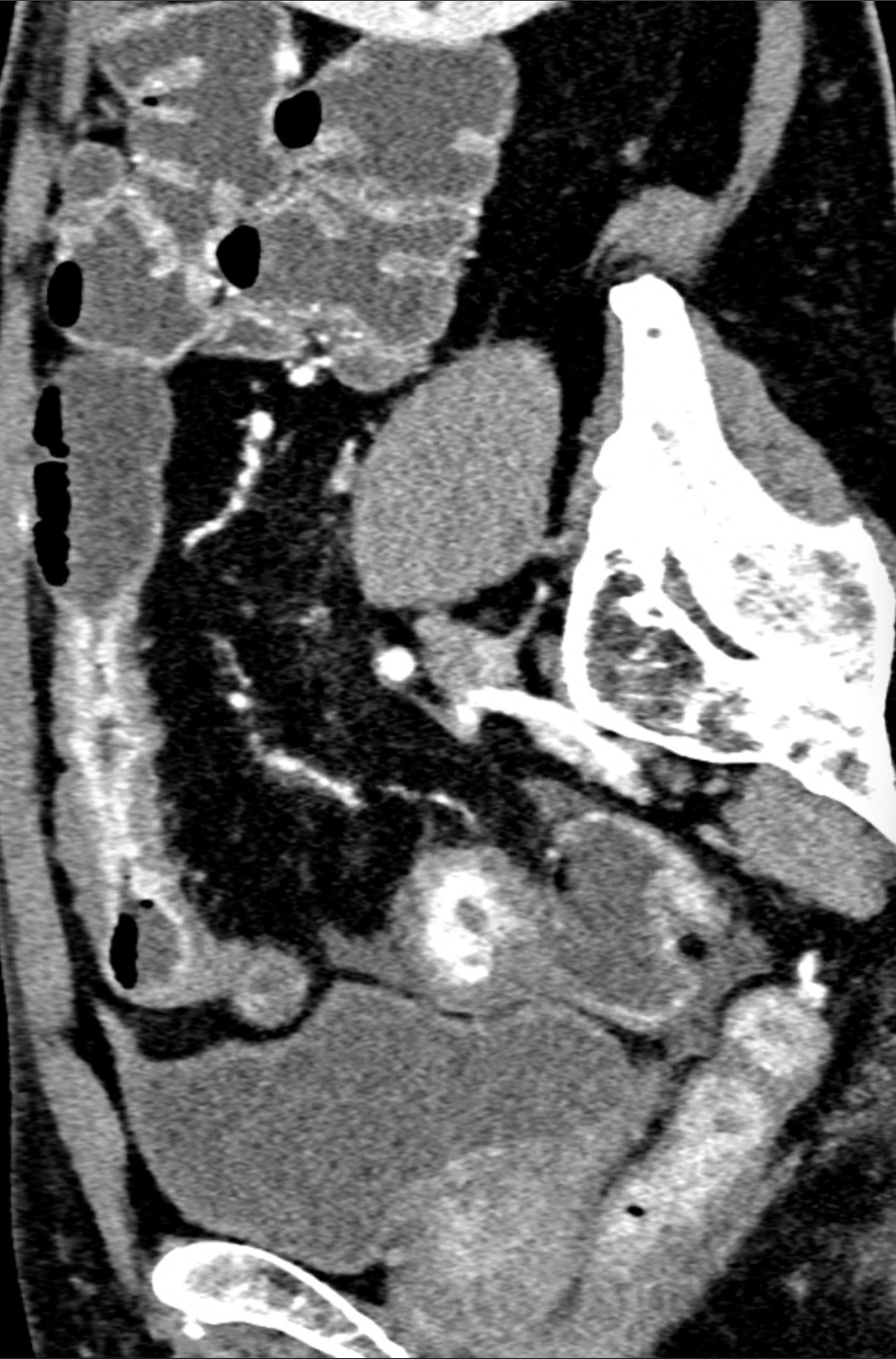
Crohn’s disease is named after the author who described it in 1932. However, there are descriptions of some clinical conditions that show that it was known as a separate disease before, for example from the descriptions of the illness of King Louis XIII of France, whose doctors described his disease with diarrhoea and perineal abscesses at the age of about 20 years. Crohn’s disease occurs in any part of the digestive tract, including rare occurrences in the tracheobronchial tree. It is most common in the small intestine (40%), in 30% of cases it occurs simultaneously in the small intestine and large intestine. The lesions that skips certain sections are typical. In the chronic stage, the strictures of the intestine are present. The earliest stage of Crohn’s disease is affliction of the typical aphthous ulcers, followed by August ulceration and the formation of a relief of cobblestones on mucosis. It is also typical for Crohn’s disease that deep ulcerations, fistulas with the surrounding intestine, and bladder, for example, but also abscesses may occur. The active disease characteristics are: a layered wall with enhancement of the mucosal and submucosal layers with submucosal edema. The strip of the edema is not present, when the disease becomes chronic, the loss of the edematous layer means, that the fibrosis occurs. On the cross-section, there is a symptom of a target, on the longitudinal section, a comb-like accentuation of the mesentery vessels under the image of the comb (comb sign)
Naeotom Alpha Peak, University Hospital Pilsen, Czechia






Comments are closed.